Kristin Everhart, MSN, ARNP, FNP-C
\
Apr 7, 2026

Three domains control your FNP exam outcome: cardiology (15-20% of exam), pharmacology (25-30%), and endocrinology (12-15%). Together, they represent 52-65% of your entire exam. If you score 70% on these three domains, your overall exam score is approximately 75% (failing). If you score 85% on these domains, your overall score jumps to approximately 86% (passing). These three domains are where exams are won and lost. Candidates who master cardiology, pharmacology, and endocrinology typically score 85%+. Candidates who struggle with any of these three typically score below 80%. There is no pathway to certification that doesn't go through these domains.
Key Insight: Cardiology, pharmacology, and endocrinology aren't harder than other domains because they're conceptually complex. They're harder because they're high-yield, they require mechanistic reasoning rather than pattern recognition, and they demand integration of clinical knowledge with guideline-based management under time pressure. The FNP exam weights these domains heavily precisely because they're foundational to primary care practice. Mastering them requires systematic study of mechanisms, high-yield drug classes and interactions, and clinical decision-making frameworks for common presentations and complications.
Cardiology: The Foundation of Primary Care Assessment
Hypertension, dyslipidemia, heart failure, and coronary artery disease account for approximately 40% of all primary care visits. The FNP exam tests your ability to manage these conditions using current guidelines. The challenge isn't understanding that statins lower cholesterol—it's knowing which statin for which patient, what LDL target to use, which patient needs high-intensity vs. moderate-intensity therapy, and what to do when standard therapy fails.
Must-Know Drug Classes in Cardiology
Drug Class | High-Yield Mechanism | Indications | Critical Contraindications | Monitoring Parameter |
|---|---|---|---|---|
ACE Inhibitors | Blocks angiotensin II → vasodilation, reduces aldosterone → less fluid retention | HTN, HF, post-MI, CKD proteinuria | K+ >5.0 mEq/L, ACE-inhibitor cough (2-10% incidence), pregnancy, bilateral RAS | K+, creatinine, BP; monitor for persistent dry cough |
ARBs | Blocks angiotensin II receptor (same effect as ACE-I but no bradykinin, so no cough) | HTN (especially with cough on ACE-I), HF with reduced EF, diabetes proteinuria | K+ >5.0, pregnancy, CKD with eGFR <30 (relative), bilateral RAS | K+, creatinine, BP |
Beta-Blockers | Decreases HR and contractility → reduces cardiac O2 demand; reduces renin release | HTN, CAD, post-MI, HF reduced EF, arrhythmias | Asthma/COPD (relative), bradycardia, 2nd/3rd degree AV block, decompensated HF (initial) | HR, BP; assess for fatigue, sexual dysfunction, worsening of asthma |
Calcium Channel Blockers (Dihydropyridine) | Blocks L-type calcium channels in vascular smooth muscle → vasodilation, reduces BP | HTN, CAD (for amlodipine), no HF benefit | HF with reduced EF (dihydropyridines), severe aortic stenosis, hypotension | BP, HR, peripheral edema (common with amlodipine) |
Thiazide Diuretics | Blocks Na-Cl cotransporter → increased Na/K excretion, volume depletion | HTN (first-line), edema, HF | Hypokalemia, hyponatremia, hyperglycemia, hyperuricemia, gout, hypercalcemia | K+, Na+, glucose, uric acid; assess for gout exacerbation |
Statins | Inhibits HMG-CoA reductase → LDL synthesis reduction; anti-inflammatory effects | Hyperlipidemia, CAD, diabetes, 10-year ASCVD risk ≥7.5% (per ACC) | Active liver disease, concurrent strong CYP3A4 inhibitors (depending on statin type), pregnancy | Lipid panel, LFTs, muscle symptoms (CK if symptomatic) |
Guideline-Based Decision Making: When Do You Escalate Therapy?
Hypertension Management (JNC-8 Guidelines): Treatment targets vary by age and comorbidity. For most adults <60 years, target BP <140/90 mmHg. For adults ≥60 years, target <150/90 mmHg. For patients with CKD (eGFR <60) or diabetes, target <140/90 mmHg. These specific targets are commonly tested. If you see a question asking about BP targets and you're unsure, the safest answer is usually 140/90 for most populations.
When to escalate from single-agent therapy: After 2-3 weeks on monotherapy at moderate-to-high dose without adequate response, add a second agent. Don't increase the first agent dose indefinitely. Combination therapy is more effective than high-dose monotherapy. Common combinations: ACE-I + thiazide, ARB + thiazide, calcium channel blocker + ACE-I.
Dyslipidemia Management (ACC/AHA 2018 Guidelines): Don't memorize exact LDL targets—they're changing. Instead, understand risk categories. Primary prevention: 10-year ASCVD risk <5% doesn't require statin therapy. 5-7.5% requires clinical judgment. ≥7.5% should receive statin. Secondary prevention (known CAD, prior MI, stroke): all patients receive statin therapy, high-intensity (atorvastatin 40-80 mg or rosuvastatin 20-40 mg). If LDL not at goal despite statin (usually <70 mg/dL in CAD), consider ezetimibe (Zetia) addition or PCSK9 inhibitor.
Heart Failure Management: Systolic vs. diastolic makes a critical difference. Reduced EF (HFrEF, EF ≤40%): use ACE-I/ARB (or ARNI—sacubitril/valsartan), beta-blocker, aldosterone antagonist, and diuretics if fluid overloaded. Preserved EF (HFpEF, EF ≥50%): no mortality benefit demonstrated for ACE-I/ARB; manage HTN and rate control.
Pharmacology: The Mechanism-to-Practice Bridge
Pharmacology on the FNP exam isn't memorizing drug names. It's understanding mechanism, predicting effects, and recognizing contraindications in specific patient populations. Here's what failed candidates typically struggle with:
Drug interactions: You know statins lower cholesterol, but do you know that fibrates + statins increase myopathy risk? That some statins (simvastatin, lovastatin) are strong CYP3A4 substrates and interact with macrolide antibiotics? That grapefruit juice inhibits CYP3A4 metabolism? These aren't random facts—they're mechanisms that explain why drug combinations are contraindicated.
Population-specific effects: Metformin is first-line diabetes therapy, but it's contraindicated in acute kidney injury (lactic acidosis risk from renal clearance impairment). ACE inhibitors are protective in diabetic nephropathy, but hyperkalemia risk is highest in CKD Stage 4-5. These population-specific contraindications are frequently tested.
Adverse effect mechanisms: Why do ACE inhibitors cause a persistent dry cough? (Bradykinin accumulation due to ACE inhibition.) Why do thiazide diuretics cause hypokalemia? (Increased distal tubule Na+ delivery drives K+ secretion.) Understanding mechanisms helps you predict and manage adverse effects.
High-Yield Pharmacology Table: Drug Interactions and Contraindications
Drug Combination | Interaction Mechanism | Clinical Result | Management |
|---|---|---|---|
ACE-I + Potassium-sparing diuretic (spironolactone) | Both increase K+ retention: ACE-I reduces aldosterone; K-sparing increases K+ reabsorption | Hyperkalemia (potentially life-threatening) | Monitor K+ closely; use with caution in CKD; many consider contraindicated together |
Statin + fibrate | Both inhibit muscle protein synthesis via different mechanisms; additive myopathy risk | Rhabdomyolysis, acute kidney injury | Avoid combination if possible; if necessary, use lowest statin dose and monitor CK closely |
Metformin + contrast dye (IV) | Metformin accumulates when renal perfusion is reduced; lactic acidosis from metformin accumulation | Lactic acidosis (especially if acute kidney injury develops post-contrast) | Hold metformin 48 hours before contrast, resume after renal function confirmed stable |
Levothyroxine + calcium, iron, PPIs | These bind levothyroxine, reducing absorption from GI tract | Decreased levothyroxine bioavailability; hypothyroid symptoms despite adequate dosing | Separate dosing by 4+ hours; monitor TSH; may require higher levothyroxine dose |
NSAIDs + ACE-I in CKD | NSAIDs reduce renal perfusion; ACE-I reduces efferent arteriole vasoconstriction; combined = severe renal perfusion reduction | Acute kidney injury, hyperkalemia | Avoid combination in CKD; use alternative analgesia; if necessary, monitor K+ and creatinine closely |
Warfarin + NSAIDs | NSAIDs inhibit platelet function; warfarin inhibits clotting factor synthesis; additive bleeding risk | GI bleeding, intracranial bleeding | Avoid; use alternative analgesia (acetaminophen); if necessary, closely monitor INR |
Endocrinology: Common Conditions and Evidence-Based Management
Type 2 diabetes management, hypothyroidism, and hyperthyroidism are foundational endocrine conditions. The challenge isn't recognizing them—it's managing them using current guidelines and avoiding common pitfalls.
Type 2 Diabetes: Management Algorithm
Initial Management (ADA 2024 Guidelines): After diagnosis, initiate lifestyle modification (diet, exercise, weight loss). Consider metformin as first-line pharmacotherapy if HbA1c ≥7% despite lifestyle modification. If eGFR ≥45 (normal or mild renal function), metformin is generally safe. If eGFR 30-44, use caution; if <30, contraindicated.
If Monotherapy Insufficient (HbA1c Still >7% After 3 months on metformin 1000 mg BID): Choose second agent based on comorbidities. If obesity: consider GLP-1 agonist (semaglutide, liraglutide). If heart failure: consider SGLT2 inhibitor (empagliflozin, dapagliflozin). If CKD proteinuria: consider SGLT2 inhibitor. If cost-sensitive: sulfonylurea or meglitinide (but higher hypoglycemia risk). Never add insulin unless HbA1c severely elevated (>10%) or acute presentation.
Blood Pressure and Lipid Management in Diabetes: All diabetics with HTN benefit from ACE-I or ARB therapy (renoprotective). LDL targets: <100 mg/dL for most, <70 mg/dL if CAD present. All patients ≥40 years with diabetes should be on statin therapy (ADA recommendation).
Common Exam Pitfalls: A patient on metformin presents with acute kidney injury (eGFR drops from 60 to 35). The diagnosis is diabetic nephropathy progression OR acute tubular necrosis. Metformin should be held immediately to prevent lactic acidosis. Many candidates mistakenly continue metformin. Another common scenario: a diabetic with new hypertension. The correct choice is ACE-I or ARB (not just any antihypertensive) because of renal protection. Many candidates select calcium channel blocker, which is acceptable but not optimal.
Thyroid Disorders: Management and Monitoring
Condition | Diagnostic TSH/T4 Pattern | First-Line Management | Monitoring | Common Pitfalls |
|---|---|---|---|---|
Primary Hypothyroidism | TSH elevated (>4.0), Free T4 low (<0.8 ng/dL) | Levothyroxine, initial 25-50 mcg daily; titrate by 25-50 mcg every 6 weeks to TSH goal 0.5-2.5 | TSH every 6 weeks until goal, then yearly; free T4 if TSH abnormal despite stable levothyroxine | Over-treating elderly (targeting TSH <0.5 increases afib risk); under-dosing in pregnancy (need 30% higher dose); not accounting for drug interactions affecting absorption |
Hyperthyroidism (Graves) | TSH suppressed (<0.1), Free T4 elevated (>1.7 ng/dL), elevated T3 often present | Propranolol (symptom control) + PTU (blocks T4→T3 conversion and TPO synthesis) or methimazole (blocks TPO synthesis); radioactive iodine if intolerant to drugs or recurrent | Free T4 every 4-6 weeks during titration; watch for agranulocytosis (rare but serious with PTU/methimazole); TSH lags behind clinical improvement by weeks | Using beta-blocker alone (controls symptoms but doesn't lower hormone levels); expecting TSH to normalize before thyroid hormones normalize (TSH suppression persists 2-3 months even after T4/T3 normalize) |
Subclinical Hypothyroidism | TSH elevated (4.5-10), Free T4 normal (0.8-1.7) | Monitor; treat if TSH >10, symptoms present, or planning pregnancy. If treating, levothyroxine 25 mcg daily | TSH every 6-12 months; assess for symptoms (fatigue, cold intolerance, weight gain) | Over-treating (levothyroxine increases CV risk when over-dosed in elderly); not treating when planning pregnancy (increases miscarriage risk) |
Critical Exam Scenarios: A patient on levothyroxine 75 mcg daily has TSH 0.2 (suppressed) and free T4 1.8 (elevated). This is over-treatment; reduce dose. A patient started on levothyroxine returns 4 weeks later with TSH still elevated. Don't increase dose yet—levothyroxine has a 6-week half-life; recheck at 6 weeks. A pregnant woman with hypothyroidism needs 30% higher levothyroxine dose due to pregnancy-related changes in thyroid hormone metabolism and increased fetal demands.
Clinical Decision-Making Framework: Integrating these three core domains
The most challenging exam questions integrate all three domains. Consider this real scenario: A 58-year-old diabetic with hypertension and dyslipidemia on metformin 1000 BID, lisinopril 20 daily, atorvastatin 40 daily presents with new persistent dry cough and K+ 5.3 mEq/L. What do you do?
Cardiology reasoning: HTN controlled (assuming cough isn't from BP elevation), dyslipidemia managed. Lisinopril is appropriate (renal protection in diabetic).
Pharmacology reasoning: ACE inhibitor-induced cough (incidence 2-10%). K+ 5.3 is mildly elevated; ACE-I increases K+ reabsorption, and diabetes increases hyperkalemia risk (impaired renal K+ excretion). The combination of ACE-I cough + mild hyperkalemia suggests ACE-I intolerance.
Clinical decision: Switch from lisinopril to ARB (equal BP/renal protection but no cough because no bradykinin accumulation). Monitor K+ in 1 week. If K+ remains elevated, consider adding low-dose thiazide to increase K+ excretion, or dietary K+ restriction.
This question tests your integration of pharmacology (why ACE-I causes cough), cardiology (appropriate agent choice for diabetic HTN), and endocrinology (hyperkalemia risk in diabetes). Many candidates would stop lisinopril and add a calcium channel blocker instead. That's pharmacologically reasonable for the cough, but clinically suboptimal because CCBs don't provide renal protection that diabetics need.
High-Yield Clinical Presentation-to-Diagnosis Table
Presentation | Key Findings | Likely Diagnosis | Evidence-Based Management | Common Exam Mistakes |
|---|---|---|---|---|
Chest pain, left arm radiation, diaphoresis, SOB | EKG shows ST elevation in anterior leads; troponin elevated | Acute anterior MI | Aspirin, clopidogrel (or ticagrelor), unfractionated heparin, consider PCI/catheterization | Giving only aspirin without P2Y12 inhibitor; delaying intervention thinking stable angina; missing STEMI and treating as unstable angina |
Fatigue, weight gain, cold intolerance, dry skin, constipation | TSH elevated (>4.0), Free T4 low | Hypothyroidism | Levothyroxine initiate 25-50 mcg daily; titrate to TSH goal 0.5-2.5 mIU/L | Starting high dose levothyroxine in elderly (cardiac risk); not checking TSH baseline; starting levothyroxine in subclinical hypothyroidism (TSH elevated, free T4 normal) without indication |
Polyuria, polydipsia, weight loss, elevated glucose (>250) | HbA1c >7%, elevated fasting glucose; UA shows glycosuria; no ketonuria | Type 2 Diabetes (hyperglycemic hyperosmolar state if severe) | Metformin first-line; lifestyle modification; target HbA1c <7% | Starting insulin immediately (insulin is not first-line); not screening for complications (neuropathy, retinopathy, nephropathy); missing microalbuminuria (indicates need for ACE-I) |
Tremor, palpitations, heat intolerance, anxiety, weight loss despite appetite | TSH suppressed (<0.1), Free T4 elevated; elevated T3 | Hyperthyroidism (Graves most likely if diffuse goiter and exophthalmos) | Propranolol for symptoms + PTU (or methimazole) to lower hormone levels; consider radioactive iodine | Using beta-blocker only (controls symptoms but doesn't address underlying pathology); expecting TSH to normalize before thyroid hormones do (TSH normalizes last) |
Dyspnea, orthopnea, PND, edema, elevated JVP | Echocardiogram shows EF <40%; BNP elevated; CXR shows pulmonary edema | HFrEF (systolic heart failure) | ACE-I/ARB, beta-blocker, diuretics if fluid overload, aldosterone antagonist; avoid NSAIDs | Not using ACE-I/ARB (mortality benefit in systolic HF); using calcium channel blocker instead of beta-blocker; not monitoring potassium on ACE-I |
Mastering the Integration: A 12-Week Deep-Dive Strategy
Weeks 1-2 (Foundation): Master basic mechanisms. For each major drug class (ACE-I, statins, metformin, levothyroxine), understand mechanism, indications, and contraindications. Create one-page reference sheets.
Weeks 3-4 (Application): Apply mechanisms to clinical scenarios. When you see "hypertensive diabetic patient," practice selecting ACE-I reasoning from renal protection, not just BP control. When you see "elevated cholesterol post-MI," select statin-based on both lipid lowering and post-MI benefit.
Weeks 5-6 (Integration): Study real cases that integrate cardiology + pharmacology + endocrinology. A 62-year-old with HTN, diabetes, and dyslipidemia on atorvastatin + metformin + lisinopril develops hyperkalemia (K+ 5.4). What's your next step? This requires understanding diabetes-related hyperkalemia risk (endocrine), ACE-I effects on K+ (pharmacology), and appropriate management (cardiology guideline).
Weeks 7-12 (Mastery): Full-length practice exams with emphasis on questions mixing cardiology, pharmacology, and endocrinology. Track your accuracy on integrated questions. If <75% on integrated questions by week 10, shift 30% of study time to integrated case practice.
Mastery Insight: The difference between 80% and 90% accuracy on cardiology/pharmacology/endocrinology questions isn't deeper content knowledge—it's the ability to recognize when domains integrate and make decisions at that intersection. A patient presenting with one symptom might require cardiology reasoning, but management involves pharmacology contraindications and endocrine comorbidity considerations. Mastery means seeing those intersections and reasoning through them systematically.
Keep Reading
Mastering these three domains is the foundation for exam success. Connect this to evidence-based preparation methodology: use spaced repetition, active recall, and clinical vignette practice specifically for these high-yield areas content to move from 70% to 85% in these critical domains.
Strategy Reminder: These domains are challenging because they require integration, not because they're inherently complex. Review how clinical experience can create false confidence in areas like cardiology management, then use targeted study to close the systematic knowledge gaps.
The Bottom Line: 52-65% of Your Exam Hinges on Three Domains
Cardiology, pharmacology, and endocrinology determine your outcome. Master them through systematic mechanism study, integration practice, and guided clinical reasoning. Don't memorize drug names or isolated facts. Instead, understand mechanisms (why ACE-I causes cough, why statins lower cholesterol, why metformin is contraindicated in kidney disease), predict effects (hyperkalemia risk with ACE-I + potassium-sparing diuretic), and apply evidence-based guidelines (ACC/AHA for cardiology, ADA for diabetes, appropriate TSH targets for thyroid management).
Every hour spent mastering these three domains yields exponential returns on your exam score. Every hour spent on other domains, when these three remain weak, is wasted effort. Prioritize ruthlessly. Audit your current knowledge in these three domains using practice questions. If you're scoring <75% in any of these three, make them your primary focus for weeks 5-8. Your outcome depends on it.
Final Word
The FNP exam respects knowledge depth in the domains that matter most. these core specialties aren't harder than other domains—they're more consequential. A mistake on a rare respiratory condition costs you one question. A mistake on cardiology or pharmacology costs you multiple questions because those concepts are woven throughout the exam. Invest disproportionate effort into these three domains. Master their mechanisms. Practice their application. Integrate them in case-based reasoning. Your 86% passing score is built on the foundation of 85%+ accuracy in these critical domains. Everything else is supplementary.
NCLEX Mastery
\
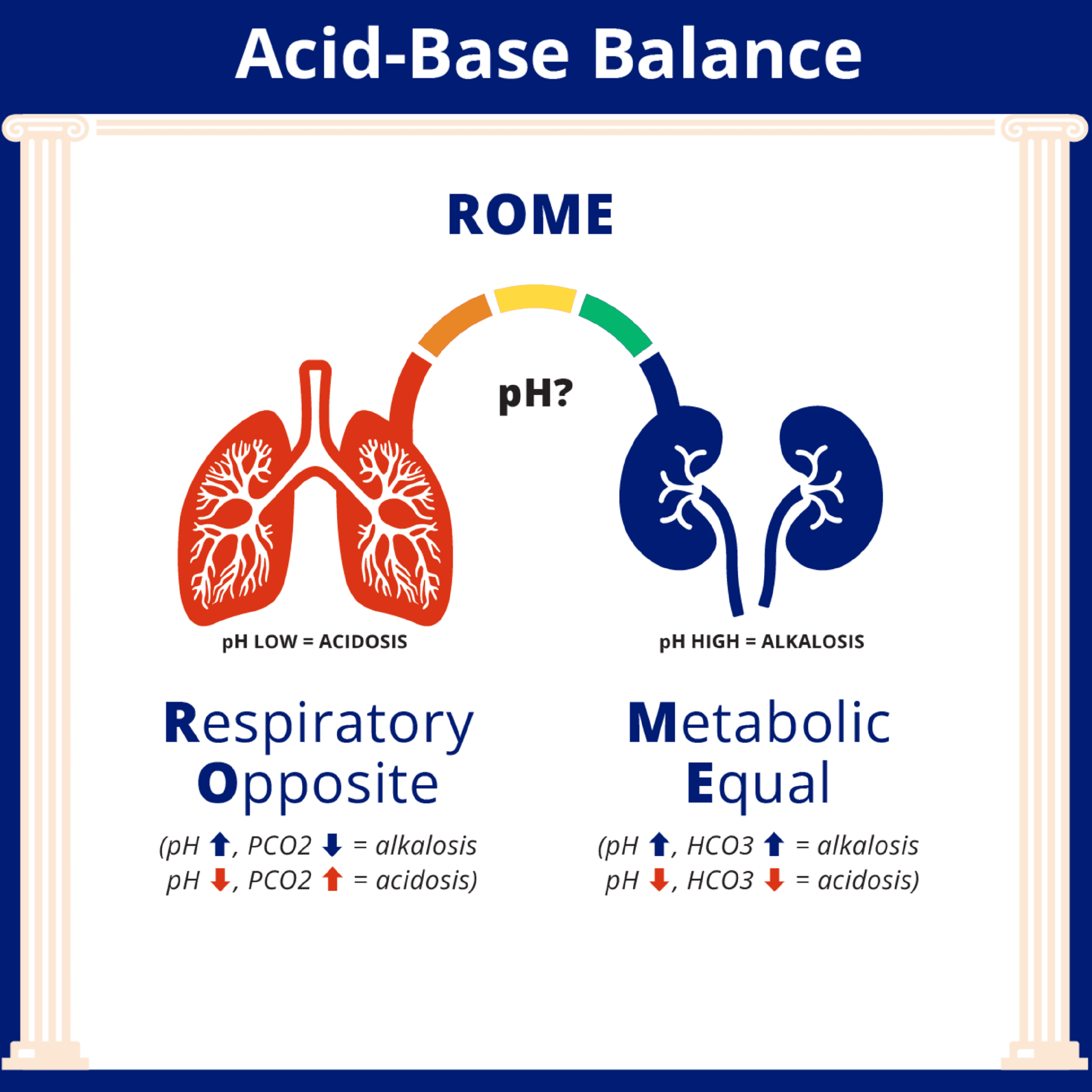
How to Interpret ABGs for the NCLEX
How to Interpret ABGs for the NCLEX

NCLEX Mastery
\
Estimating TBSA: What Every Nurse Should Know
Estimating TBSA: What Every Nurse Should Know

Catherine Cantrell, MSN, RN
\
What Actually Happens When You Fail a Nursing Course




