Kristin Everhart, MSN, ARNP, FNP-C
\
Apr 7, 2026

Three weeks before the AGNP exam, you're working through practice questions and hit a vignette: "An 82-year-old man presents with fatigue and shortness of breath for 2 days. Vital signs: HR 98, BP 140/88, RR 22, O2 sat 93% on room air. He denies chest pain. EKG shows no acute changes. Troponin negative. Which is the most likely diagnosis?" You pick heart failure. Wrong. The answer is silent myocardial infarction—the EKG can be normal in elderly MI, troponin negative in the first few hours, and the presentation is fatigue and dyspnea, not classic chest pain. You close the laptop, frustrated. Nobody taught you that.
This is the core challenge of AGNP exam preparation: geriatrics rewrites the rules. The pathophysiology you learned in undergrad—classic presentations, textbook findings, standard diagnostic criteria—doesn't apply the same way to patients over 65. And your program, designed for nurses entering practice, often spends 20% on geriatrics and 80% on general adult medicine. The exam is the inverse.
This guide identifies the 5 most common challenges AGNP students face, explains why they happen, and provides evidence-based solutions to overcome them. These aren't knowledge gaps you can close with more questions. These are conceptual shifts you must make to think like a geriatric clinician.
Key Insight: AGNP students struggle not because they lack intelligence or work ethic. They struggle because geriatrics requires learning a new clinical language—a language where your foundational nursing knowledge is partially wrong. A normal troponin doesn't rule out MI. A normal CBC doesn't mean no infection. A "cognitive screening" that's normal doesn't mean no dementia. Accepting this—that you must unlearn and relearn—is the first step to mastery.
Challenge 1: Geriatric Polypharmacy and Medication Complexity
The average 75-year-old takes 5-6 medications. The average 85-year-old takes 8-10. By 95+, patients often take 12+ medications. Each medication was prescribed for a good reason. But together, they create a pharmacological minefield where drug-drug interactions, age-related metabolism changes, and polypharmacy side effects become the primary disease.
The Core Problem: You can memorize every drug in Beers Criteria, know every black box warning, and still miss the medication problem because the questions aren't asking "Is this drug inappropriate?" They're asking "Why is this 78-year-old confused?" The answer is: his five blood pressure medications are over-treating him. His systolic BP is 110 and he's on lisinopril, metoprolol, amlodipine, and hydrochlorothiazide. He's hypotensive and confused. The fix: stop two medications and recheck his cognition in a week.
Why It's Hard: Your pharmacy education taught you: lisinopril is indicated for hypertension. But in a 78-year-old with baseline BP 120/70, lisinopril is contraindicated—tight BP control (systolic <130) increases fall risk and mortality in very elderly. Your knowledge is right; the application changes with age. Every medication needs this dual analysis: Is it right for a younger adult? Is it still right for a 78-year-old?
Medication Class | Younger Adult Logic | Elderly Logic | Exam Question Pattern |
|---|---|---|---|
Benzodiazepines | Excellent for acute anxiety; short-term use is safe | Cause delirium, falls, fractures, addiction even at low doses; avoid entirely | Pt on alprazolam has a fall → identify benzo as cause → deprescribe |
Anticholinergics | Useful for OAB, Parkinson's; side effects are minor | Worsen cognition, urinary retention, constipation, falls significantly | Pt on diphenhydramine has confusion → identify anticholinergic → switch to SSRI |
Antihypertensives (Aggressive) | Tight control reduces MI and stroke risk | Tight control increases falls, syncope, AKI, mortality (paradoxically) | Pt on 4 BP meds with SBP 110 has syncope → deprescribe 1-2 agents |
NSAIDs (Chronic) | Usually safe for acute pain; chronic use is a trade-off | High GI bleed, AKI, hyperkalemia risk; almost always contraindicated | Pt on HCTZ, ACE-I, chronic ibuprofen develops AKI → identify NSAID + CKD |
Opioids | Potent pain relief; risk-benefit usually favors use | Overdose risk, respiratory depression, delirium, constipation, falls; reserve for cancer pain | Pt on morphine, hydrocodone, tramadol with oversedation → deprescribe opioids |
Solution: Build a Polypharmacy Decision Framework
For every medication in an elderly patient's list, ask four questions: (1) Is the indication clear and current? (2) Is the dose appropriate for age/renal function? (3) Are there safer alternatives? (4) Are there drug-drug interactions? If you answer "no" to 1-3 or "yes" to 4, the medication is a candidate for deprescribing or change. Practice this framework on every complex polypharmacy question. By exam day, it should be automatic.
Second: memorize the top 15 drug-drug interactions in elderly. Not all interactions—the 15 most common and dangerous. (1) ACE-I + potassium-sparing diuretic + NSAID = hyperkalemia and AKI. (2) Warfarin + NSAID = GI bleed. (3) Digoxin + thiazide diuretic (hypokalemia) = digoxin toxicity. (4) Metformin + contrast dye = acute kidney injury. (5) Clopidogrel + omeprazole (CYP2C19 inhibition) = reduced antiplatelet effect. Master these 15. You'll see them repeatedly on the exam.
Challenge 2: Atypical Presentations of Common Acute Illnesses
A 65-year-old having a heart attack often presents with chest pain, diaphoresis, and dyspnea. An 82-year-old having a heart attack often presents with fatigue, weakness, and dyspnea—no chest pain at all. An 45-year-old with pneumonia has fever, cough, and purulent sputum. A 78-year-old with pneumonia often has normal temperature, minimal cough, and just confusion and falls.
The Core Problem: Atypical presentations in elderly are not rare exceptions. They are the norm. Your brain was trained on textbooks written for younger populations. The AGNP exam expects you to recognize that elderly patients present atypically—and to suspect acute illness in the absence of classic symptoms.
Why It's Hard: Your prior learning created pattern matching: chest pain = cardiac. Fever + cough = pneumonia. Dysuria = UTI. But elderly medicine says: fatigue = cardiac (or many other things). Confusion = infection (or medications, or metabolic, or baseline). Falls without trauma = acute illness (until proven otherwise). The patterns are weaker and more inclusive. You must learn to think probabilistically: "What serious illnesses could cause fatigue and dyspnea in an 82-year-old?" and then methodically rule them out.
Classic Presentation | Elderly Atypical Presentation | Why It Happens | Exam Implication |
|---|---|---|---|
MI: Chest pain, diaphoresis, dyspnea | MI: Fatigue, dyspnea, weakness; no chest pain | Blunted pain perception (neuropathy, cognitive changes); confused pain interpretation | Troponin can be negative early; normal EKG possible; suspect based on dyspnea alone |
Pneumonia: Fever, productive cough, pleurisy | Pneumonia: Confusion, falls, tachypnea, no fever or cough | Blunted fever response; weak cough reflex; aspiration risk | Absence of fever doesn't rule out pneumonia; confusion is a cardinal sign in elderly |
UTI: Dysuria, frequency, urgency | UTI: Confusion, incontinence, falls; no dysuria | Cognitive impairment prevents reporting dysuria; atrophy of urethra changes sensation | Asymptomatic bacteriuria is NOT UTI; confused elderly patient = assume UTI until proven otherwise |
Sepsis: Fever, tachycardia, rigors | Sepsis: Hypothermia, bradycardia (in some), confusion, hypotension | Blunted inflammatory response; altered thermoregulation; delayed immune response | Temperature <96.8 in septic elderly is worse than fever; confusion is earliest sign |
Hypoglycemia: Tremor, diaphoresis, anxiety | Hypoglycemia: Confusion, falls, weakness; no tremor/diaphoresis | Autonomic neuropathy from chronic diabetes blunts adrenergic symptoms | Check glucose in confused elderly patient regardless of diabetes history |
Depression: Sad mood, anhedonia | Depression: Fatigue, cognitive impairment ("pseudodementia"), no sadness reported | Cognitive symptoms predominate; patients may deny mood changes | Cognitive impairment + negative mood on PHQ-9 = depression until proven otherwise |
Solution: Study Atypical Presentations Explicitly
Don't just read disease chapters. Read a geriatric medicine textbook chapter (Ouslander, Hazard, Essentials of Clinical Geriatrics) that specifically addresses how presentations change with age. For each major disease (MI, pneumonia, UTI, sepsis, stroke, hypoglycemia, depression), write out: Classic presentation → Atypical elderly presentation → Diagnostic pearls. Then do 50-100 vignettes where you practice recognizing disease without classic symptoms.
Second: memorize the principle: "Confusion is always pathology until proven otherwise." In younger adults, we ask "Is the patient oriented?" In elderly, we ask "Is the patient MORE confused than baseline?" Acute confusion (delirium) is a sign of acute illness—infection, medication toxicity, metabolic derangement, acute stroke, MI, or other serious pathology. When you see a vignette: "78-year-old normally independent, now confused for 3 days," your first differential is: infection, medications, metabolic derangement, stroke, MI, hypoxia. Classic delirium workup: CBC, metabolic panel, UA+culture, blood cultures, CXR, CT head.
Challenge 3: Cognitive Changes, Dementia, and Normal Aging
An 80-year-old comes in to your clinic. She reports she's "getting forgetful." Her daughter says she gets lost driving home sometimes and forgets conversations they had last week. You screen her with the Montreal Cognitive Assessment (MoCA) and she scores 26/30—the cutoff for normal is typically 26, so she "passes." Do you reassure her that she's cognitively normal? Wrong. She probably has mild cognitive impairment (MCI) or early dementia, and you missed it.
The Core Problem: Screening tests (MoCA, Mini-Cog, Montreal) have cutoffs designed to detect moderate to severe cognitive impairment, not early decline. Many elderly patients with MCI pass these screens. The exam expects you to go beyond screening—to understand the difference between normal aging, MCI, and dementia; to assess functional decline (Can she still manage medications? Pay bills? Drive safely?); and to recognize that a positive screen needs follow-up, not reassurance.
Why It's Hard: You learned: Screen with validated tool → Score normal → Patient reassured. But geriatrics says: Screen with validated tool → Score borderline or normal → Assess functional decline → Get collateral history from family → Likely has early dementia → Refer for neuropsych testing. The screening is just the start, not the answer.
Normal Aging vs. Pathology (Key Distinctions):
Normal Aging (Does NOT Require Intervention): Slow processing speed (takes longer to recall information); minor word-finding difficulty (occasional "tip-of-the-tongue" moments); taking longer to learn new information; occasional forgetfulness of less important details; able to function independently in all activities of daily living (ADLs) and instrumental ADLs (IADLs—managing money, medications, transportation).
Mild Cognitive Impairment (Requires Follow-up): Noticeable memory loss beyond normal aging (family/self-reported); difficulty with complex tasks (paying bills, managing medications); getting lost in familiar places; difficulty completing familiar tasks; but still independent in basic ADLs; screening tests may be normal or borderline; functional decline noted by informant.
Mild-to-Moderate Dementia (Requires Investigation & Management): Significant memory loss; difficulty recognizing familiar people or places; needs reminders for medications and appointments; difficulty with complex conversations; behavioral changes (sundowning, agitation); dependence in some IADLs and potentially ADLs; screening tests abnormal; significant functional decline.
Solution: Learn the Functional Assessment Questions
Go beyond screening tests. Ask: (1) "Can you manage your medications without help?" (2) "Can you manage your finances—pay bills, balance checkbook?" (3) "Can you shop and prepare meals?" (4) "Can you do your housework?" (5) "Can you drive safely and get around the community?" (6) "Do you need someone to remind you of appointments?" Functional decline in any of these = cognitive impairment, even if screening test is borderline.
Second: always get collateral history from family. Ask the family member: "Compared to 2-3 years ago, is she more forgetful? Does she repeat conversations? Get lost? Struggle with tasks she used to do easily?" A family-reported decline trumps a screening test score. Document it. If functional decline is present, refer for neuropsych testing to distinguish MCI from early dementia.
Third: understand that depression and cognitive impairment overlap in elderly. Depression can cause pseudodementia (cognitive symptoms that resolve when depression is treated). Cognitive impairment can cause depression (adjustment to declining function). Always screen for depression (PHQ-9) in cognitively impaired patients. If both are present, treat depression first, then reassess cognition in 6-8 weeks.
Challenge 4: Geriatric-Specific Guidelines and Evidence-Based Medicine Applied to Older Adults
You learned: Blood pressure target is <130/80 for all adults (per ACC/AHA 2017 guidelines). But an 82-year-old with prior stroke and baseline BP 135/78 started on aggressive antihypertensive therapy becomes syncope-prone and confused. The SPRINT trial (which drove the <130 target) excluded adults >75 and those with prior stroke. The current evidence for your patient says: target 130-150 systolic, accept diastolic 70-80, prioritize avoiding hypotension over achieving strict numbers. The guideline you memorized is wrong for your patient's age.
The Core Problem: Major clinical guidelines (for HTN, diabetes, lipids, anticoagulation, screening) are based on trials mostly including adults <75. When you apply those guidelines to patients >75-80-85, you're extrapolating beyond the evidence. The AGNP exam expects you to know which guidelines apply fully, which need modification, and which are explicitly contraindicated in very elderly.
Why It's Hard: You trust guidelines. You should—they're evidence-based. But they're also population-based. A guideline that benefits the average 60-year-old may harm the average 85-year-old. You must learn to ask: "Does the evidence apply to this patient's age group? What is the patient's life expectancy? What are their goals of care?" and then adapt the guideline.
Clinical Goal | Standard Guideline | Geriatric Modification (75+) | Very Elderly Modification (85+) |
|---|---|---|---|
Hypertension Target | BP <130/80 (ACC/AHA 2017) | BP 130-150 systolic acceptable; avoid hypotension and syncope | BP 140-150 systolic often preferred; deprioritize antihypertensives if causing falls/confusion |
Diabetes Glycemic Target | A1C <7% (ADA) | A1C 7-8% reasonable; avoid hypoglycemia intensely (causes falls, delirium, MI) | A1C 7.5-8% acceptable; no aggressive treatment |
LDL-Cholesterol Target | LDL <70 for CAD (ACC/AHA) | LDL <70 reasonable if on statin; avoid intensive statin if not already on | Statin benefit unproven if not already established; no new statin initiation |
Anticoagulation for AFib | CHADS2-VASc ≥1 = anticoagulate (AHA/ACC) | Yes, anticoagulate; high bleed risk but stroke risk higher | Individualize; assess fall risk, renal function, medication interactions; DOACs preferred over warfarin |
Cancer Screening | Mammography to 75; colonoscopy to 75-85 | Screening appropriate if life expectancy >7-10 years and will change management | Screening rarely beneficial; deprioritize unless acute finding |
Solution: Internalize the Life-Expectancy Question
For every treatment decision, ask: "What is this patient's life expectancy?" U.S. life expectancy at age 65 is ~18 years. At 75: ~11 years. At 85: ~6.5 years. At 95: ~3.5 years. Then ask: "Will this treatment benefit the patient within their life expectancy?" A 88-year-old with life expectancy 5 years probably doesn't benefit from starting a statin (which takes 3-5 years to prevent MI). An 82-year-old with prior MI and life expectancy 10 years probably should stay on statin. This calculus is geriatric-specific and rarely tested in younger populations.
Second: understand SPRINT and ACCORD and understand their limitations. SPRINT (tight BP control) excluded >75. ACCORD (intensive glucose control) found no MI benefit in type 2 diabetes. LIPITOR trials were mostly <75. These landmark trials inform guidelines but don't define truth for 85-year-olds. Know what the trial showed and who was included. Then ask: does it apply to this patient?
Third: read Choosing Wisely campaign recommendations for older adults. These are explicitly about what NOT to do—deprescribing, avoiding unnecessary tests, avoiding overtreatment. Demedicalizing is part of geriatric practice. Questions asking "What should you NOT do?" often hinge on Choosing Wisely thinking.
Challenge 5: Complex Care Coordination Across Multiple Settings
Your 77-year-old patient is admitted to the hospital with pneumonia and decompensated heart failure. She's improved on IV antibiotics and diuretics. Now she's stable enough to discharge. But she lives alone, can barely walk due to deconditioning, has early dementia, takes 9 medications, and can't afford a single medication. If you discharge her back home without a plan, she'll be readmitted within 2 weeks. The exam question asks: "What is your next step?" The right answer isn't "discharge to home." It's "arrange transitional care: home health, PT/OT, social work consultation, case management, pharmacy reconciliation, and close outpatient follow-up."
The Core Problem: Geriatric patients don't exist in isolation. They exist in complex social and medical ecosystems: multiple comorbidities, multiple medications, multiple providers, potential caregiver burnout, financial constraints, transportation barriers, social isolation, and functional decline. The AGNP exam tests your ability to coordinate care across these dimensions, not just treat the acute illness.
Why It's Hard: Most nursing training focuses on individual patient management. Geriatric care requires systems thinking—understanding how discharge decisions affect home safety, how medication changes affect caregiver burden, how social determinants affect health outcomes. These aren't skills you learned in pharmacology class. They're earned through experience and intentional study of geriatric care models.
Key Care Coordination Considerations (Exam-Tested):
Transitions of Care (Hospital → Home/Nursing Home): Medication reconciliation (ensuring discharge medications match what patient actually takes), patient/caregiver education on new medications/restrictions, follow-up appointments scheduled before discharge, clear discharge instructions, communication to outpatient provider, and consideration of transitional services (home health, PT/OT, social work).
Caregiver Assessment and Support: Is the caregiver present and able to help? What is their stress level? Do they need respite care? Can they manage medications and monitor for complications? If burden is high or caregiver absent, discharge planning changes (may need assisted living or nursing home instead of home).
Social Determinants Assessment: Does patient have safe housing? Heat in winter? Can afford medications? Transportation to appointments? Food security? Social isolation? These directly affect health outcomes. A patient with no heat, no food, and no transportation will fail at home even with the best medical plan.
Palliative Care and Goals-of-Care Conversations: For patients with limited life expectancy or multiple serious illnesses, shift from cure-focused to comfort-focused care. Ask: "If you become very ill and can't make decisions, what kind of care would matter most to you?" Discuss advance directives, DNR/DNI status, and what quality of life means. Document these conversations and honor them in care planning.
Solution: Build a Discharge Planning Checklist
Create a mental checklist for every patient discharge: (1) Medications reconciled and patient/caregiver educated? (2) Follow-up appointments scheduled and confirmed? (3) Caregiver capable and supported? (4) Social determinants assessed (housing, food, heat, transportation, social connection)? (5) Functional needs met (PT/OT, home health, assistive devices)? (6) Goals of care documented? (7) Red flags reviewed (what symptoms should prompt ED visit?)? If any are unchecked, your discharge plan is incomplete.
Second: understand the spectrum of living situations for elderly. Independent living (patient alone or with spouse) requires high function and support system. Assisted living (meals provided, medication management available, some supervision) suits moderate impairment. Nursing home suits high care needs. Memory care suits dementia. Skilled nursing facility (SNF) suits post-acute illness recovery. Hospice suits end-of-life comfort care. The exam will ask you to match patient acuity/function to appropriate setting.
Exam Strategy: When you see a discharge planning question, first assess: functional status, cognitive status, caregiver situation, and medical complexity. Then match to setting: independent living (high function, good cognition, strong caregiver, simple medical needs) vs. assisted living (moderate impairment, some caregiver support, multiple meds) vs. SNF (post-acute, needs therapy) vs. nursing home (can't live safely at home) vs. hospice (prognosis <6 months, comfort focus). You're matching patient to ecosystem, not just medical condition.
Comprehensive Challenge Summary: Study Priority Matrix
Challenge | Why Students Fail | Study Priority | Solution | Practice Approach |
|---|---|---|---|---|
1. Polypharmacy | Don't recognize medication interactions; miss Beers Criteria contraindications | HIGHEST - represents 25-30% of exam | Master Beers Criteria; learn top 15 drug-drug interactions; build deprescribing framework | 300+ pharmacology-specific questions focused on drug interactions and contraindications |
2. Atypical Presentations | Expect classic symptoms; miss illness without textbook signs | HIGHEST - directly tested in vignettes | Study atypical presentations explicitly (silent MI, asymptomatic UTI, low-temp sepsis); practice recognizing disease without classic signs | 100+ questions where diagnosis is not obvious from initial symptoms |
3. Cognitive Changes | Rely on screening test alone; don't assess functional decline | HIGH - frequently tested, high miss rate | Learn functional assessment; get collateral history; distinguish normal aging, MCI, dementia; screen for depression | 30-40 questions on cognitive impairment, dementia assessment, delirium |
4. Geriatric Guidelines | Apply standard guidelines to elderly patients without modification | HIGH - policy and standards frequently tested | Understand life expectancy as decision-making framework; know which guidelines change >75-85; read Choosing Wisely | 50+ questions on HTN targets, diabetes targets, cancer screening, anticoagulation in elderly |
5. Care Coordination | Focus on medical diagnosis; miss discharge planning, caregiver assessment, social determinants | MEDIUM-HIGH - represents 5-10% of exam and professional role domain | Build discharge planning checklist; assess caregiver and social support; understand living situation options; goals-of-care conversations | 20-30 questions on discharge planning, care coordination, caregiver support, goals of care |
Use this matrix to weight your study. Spend 40% of study time on polypharmacy and atypical presentations (the highest-yield, hardest areas). Spend 30% on cognitive changes and geriatric guidelines. Spend 20% on care coordination and professional role. Spend 10% on other content. This allocation matches exam weighting and student failure patterns.
Keep Reading: Deepen Your Geriatric NP Expertise
The Ultimate AGNP Exam Study Guide for 2026: Master the 12-week timeline and 2,000-question strategy that incorporates high-yield geriatric content. https://hltmastery.com/nursing/agnp/resources/agnp-exam-study-guide-2026
AGNP Pharmacology: Geriatric Drug Review: Master Beers Criteria, polypharmacy, and drug-drug interactions—the #1 challenge area for AGNP students. https://hltmastery.com/nursing/agnp/resources/agnp-pharmacology-geriatric-drug-review
AGPCNP vs AGACNP: Understand which specialty aligns with your strengths (primary care demands broad geriatric knowledge; acute care demands rapid decision-making under acuity). https://hltmastery.com/nursing/agnp/resources/agpcnp-vs-agacnp-choosing-your-specialty
AANP vs ANCC for AGNP: Choose the right exam and study accordingly. Both test geriatric knowledge; study approach differs. https://hltmastery.com/nursing/agnp/resources/aanp-vs-ancc-for-agnp-which-exam
Final Word
AGNP students struggle because geriatrics is genuinely hard. It requires unlearning the medical model you learned for younger adults and relearning a model based on complexity, function, and quality of life. You can't memorize your way through. You have to think differently.
But here's the good news: the struggles you're facing are exactly what exam makers expect. They know polypharmacy is hard. They know atypical presentations are hard. They know care coordination is hard. So they test these relentlessly. If you focus your study on the 5 challenges outlined here—and accept that mastering geriatrics takes deeper work than memorizing drug side effects—you will not just pass the AGNP exam. You will understand your patients better and provide better care.
The students who pass are the ones who accepted the challenge, studied deliberately, and thought like geriatric clinicians from day one. You can be that student.
Get the right prep plan: HLT Mastery's AGNP program is built around these 5 challenges. We focus on atypical presentations, polypharmacy mastery, geriatric guidelines, care coordination, and cognitive assessment. 400K+ nurses have trusted us to get them ready. Join our AGNP prep program—let's tackle these challenges together and get you certified.
NCLEX Mastery
\
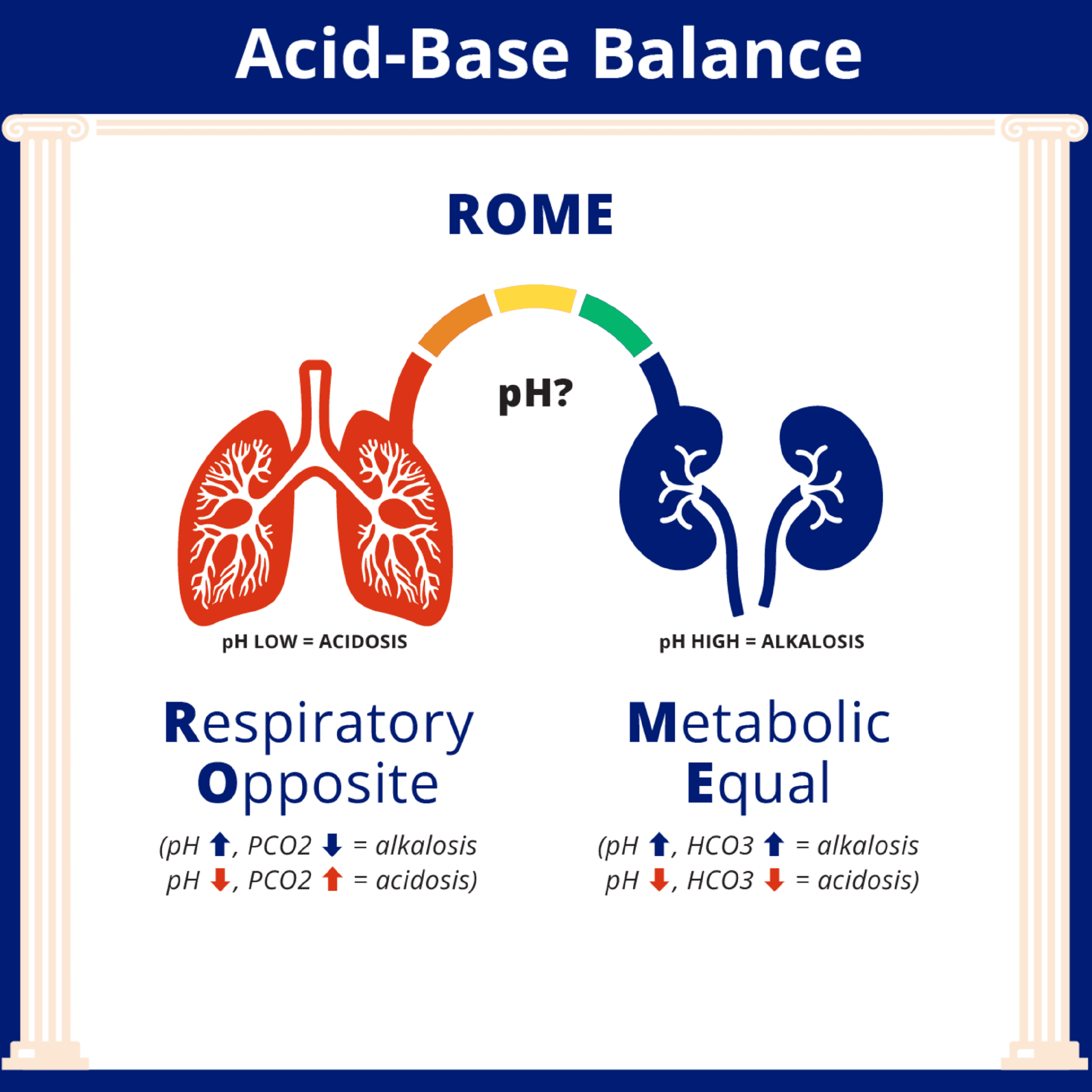
How to Interpret ABGs for the NCLEX
How to Interpret ABGs for the NCLEX

NCLEX Mastery
\
Estimating TBSA: What Every Nurse Should Know
Estimating TBSA: What Every Nurse Should Know

Catherine Cantrell, MSN, RN
\
What Actually Happens When You Fail a Nursing Course




