Kristin Everhart, MSN, ARNP, FNP-C
\
Apr 7, 2026

You're halfway through your Master's in Nursing and realize your program offers a choice: Adult-Gerontology Primary Care NP (AGPCNP) or Adult-Gerontology Acute Care NP (AGACNP). Your advisor waves a hand: "Both are marketable. Choose based on where you see yourself." But that non-answer doesn't help. The truth is, these two specialties differ in scope of practice, clinical settings, patient acuity, salary, job market demand, and—critically—the mental work you'll do every day.
This guide cuts through the vagueness. We've analyzed the certification exams, real-world scope differences, salary data from 2024-25, job market demand by region, and what your daily work actually looks like in each specialty. By the end, you'll understand not just which exam to take, but which specialty fits your clinical interests, lifestyle goals, and career trajectory.
Key Insight: AGPCNP and AGACNP are fundamentally different roles with different knowledge bases, different daily stressors, and different patient populations. The AGPCNP manages chronic disease in stable patients over months and years; the AGACNP manages acute, life-threatening conditions in hours and days. Both are essential. Neither is "better"—but one will fit you better.
Scope of Practice: Where You Treat Patients
The scope of practice distinction is the clearest dividing line between AGPCNP and AGACNP.
AGPCNP (Primary Care NP): You are the first point of contact for most patient problems. You work in outpatient settings where patients are medically stable or managing chronic disease. Your role includes health promotion, disease prevention, management of acute minor illnesses, and long-term care of chronic conditions (hypertension, diabetes, COPD, heart failure). You manage medication adjustments over time, coordinate preventive care (screenings, vaccinations), and refer to specialists when needed. You are a longitudinal provider—you see the same patient repeatedly over months and years, tracking their trajectory.
AGACNP (Acute Care NP): You manage acutely ill or injured patients in high-acuity settings. You work in ICUs, emergency departments, step-down units, or acute care floors where patients' conditions are rapidly changing. Your role includes initial stabilization, critical decision-making under time pressure, management of complex acute illnesses and complications, coordination with multiple specialists, and often anticipating deterioration before it happens. You are an episodic provider—you see a patient for days to weeks during a critical illness episode, then they transfer or discharge.
This difference shapes everything about the job. An AGPCNP managing a 72-year-old with type 2 diabetes and HTN will spend time counseling on diet, adjusting metformin dosing, discussing cardiovascular risk reduction, and planning annual screening. An AGACNP managing a 72-year-old admitted with diabetic ketoacidosis and acute kidney injury will spend time on mechanical ventilation management, insulin drips, vasopressor support, and preventing sepsis.
Clinical Settings: Where You Work Daily
Clinical Setting | AGPCNP | AGACNP | Work Pace | Patient Acuity |
|---|---|---|---|---|
Private Practice / Primary Care Clinic | Primary setting | Rare | Scheduled, predictable | Stable to mild acute illness |
Community Health Center | Primary setting | Rare | High volume, scheduled | Stable chronic disease |
Urgent Care / Walk-in Clinic | Secondary setting | Occasional | Fast-paced, unscheduled | Minor acute illness |
ICU (Medical, Surgical, Mixed) | Rare | Primary setting | Very fast, unpredictable | Critical illness |
Emergency Department | Rare | Primary setting | Chaotic, rapid triage/treatment | Acute to critical |
Hospital Step-Down Unit | Rare | Primary setting | Fast, multi-patient monitoring | Post-acute illness |
Geriatric Clinic / Specialist | Primary setting | Rare | Scheduled, consultative | Complex chronic disease |
Nursing Home / Long-Term Care | Primary setting | Rare | Scheduled, episodic | Stable with acute changes |
Home Health / Telehealth | Growing setting | Rare | Remote, scheduled | Stable chronic disease |
Notice the pattern: AGPCNP works scheduled, predictable environments where you manage ongoing relationships. AGACNP works chaotic, unpredictable environments where you handle emergencies and rapid changes.
Patient Populations: The Patients You'll See
AGPCNP Typical Patients: A 68-year-old woman with type 2 diabetes for 12 years, hypertension, hyperlipidemia, osteoarthritis, and anxiety. A 74-year-old man post-MI (2 years ago) now on beta-blocker, statin, ACE inhibitor, managing stable heart failure. An 81-year-old widow with cognitive decline, multiple medications, attending your clinic quarterly to review medications and screen for complications. These patients are medical-stable but complex. Your job is optimization—improving control of chronic disease, preventing complications, maintaining function and quality of life.
AGACNP Typical Patients: A 65-year-old admitted with community-acquired pneumonia progressing to septic shock, now on mechanical ventilation and vasopressors. A 72-year-old post-operative day 3 from hip fracture repair with acute kidney injury and altered mental status. A 78-year-old with acute decompensated heart failure and pulmonary edema in the ICU. These patients are acutely unstable, often multi-organ dysfunction, requiring rapid titration of medications and frequent reassessment.
The patient populations overlap in age (both work with older adults), but diverge sharply in acuity and timeline. AGPCNP patients live months to years with their chronic conditions; AGACNP patients live days to weeks in acute crisis.
Knowledge Requirements: What You Must Master
Domain | AGPCNP Focus | AGACNP Focus |
|---|---|---|
Pharmacology | Chronic disease management (beta-blockers for HTN, metformin for DM, statins for lipids); drug interactions in polypharmacy; deprescribing; long-term side effects | Acute illness management (vasopressors for shock, inotropes for cardiac failure, sedatives for ventilated patients); rapid titration; ICU drug protocols; acute toxicity |
Assessment | Longitudinal assessment (tracking disease progression over time); functional assessment; frailty screening; cognitive assessment for dementia | Rapid, focused assessment (is the patient stable? deteriorating?); hemodynamic assessment; respiratory assessment; neurological assessment |
Diagnostics | Interpreting screening tests; managing abnormal results; deciding when to refer to specialists; cost-effective workup | Interpreting ICU monitors; bedside ultrasound; interpreting ABGs; lactate trends; CXR/CT interpretation for acute change |
Disease Management | Chronic disease guidelines (HTN management, DM glycemic targets, COPD exacerbation prevention); preventive care; advance directives | Acute disease protocols (sepsis bundles, ventilator protocols, acute kidney injury management); complications; multi-organ failure |
Communication | Patient and family education (lifestyle, medication adherence); shared decision-making for chronic disease; longitudinal relationship-building | Rapid communication with team (rounds, handoffs); family communication during crisis; interdisciplinary coordination |
AGPCNP knowledge is deep and broad across chronic disease—you need to understand the long-term trajectory and prevention. AGACNP knowledge is deep and narrow across acute illness—you need to understand the next 24 hours and prevent deterioration. Both require geriatric expertise because age changes how you manage disease.
Job Market Demand: Where Jobs Are Growing
Job availability is a critical factor in your decision. Both specialties are in demand, but demand varies by region and setting.
AGPCNP Job Market (2024-25): High demand nationwide, especially in rural and underserved areas. Primary care NP shortages are endemic—most primary care clinics have openings for AGPCNPs. Rural health, federally qualified health centers (FQHCs), and small group practices actively recruit. Urban areas have more competition, but still growing demand. Telemedicine and home health are rapidly expanding AGPCNP roles. Rural AGPCNP jobs average 8-12 openings per available candidate; urban/suburban average 3-5 openings per candidate. Salary growth is modest (1-2% annually) but job security is high.
AGACNP Job Market (2024-25): High demand in hospitals with ICUs and emergency departments. All major health systems need AGACNPs in ICUs. Some rural hospitals lack ICUs, limiting local opportunities. Urban hospital systems have more openings but also more competition. AGACNP jobs are 70% hospital-based, limiting geographic flexibility. If you're set on a specific region without major hospitals, AGACNP jobs are scarce. Urban AGACNP jobs average 4-8 openings per candidate; rural average 1-2 (often zero). Salary growth is faster (2-3% annually) but job availability is concentrated geographically.
Career Flexibility: An AGPCNP credential gives you flexibility—you can work in primary care, urgent care, occupational health, geriatric clinics, nursing homes, telehealth, research, or education. An AGACNP credential is more niche—ICU, ED, or acute care floors are your primary options. If career mobility and geographic flexibility matter to you, AGPCNP is the safer bet.
Salary Comparison: What You'll Earn
Years of Experience | AGPCNP Salary | AGACNP Salary | Difference | Job Availability |
|---|---|---|---|---|
0-2 years (new grad) | $105,000 - $125,000 | $115,000 - $140,000 | +$10-15K for AGACNP | AGPCNP: more openings nationally |
3-5 years | $115,000 - $140,000 | $130,000 - $165,000 | +$15-25K for AGACNP | AGACNP: faster salary growth |
6-10 years | $125,000 - $155,000 | $150,000 - $190,000 | +$25-35K for AGACNP | AGPCNP: more flexible options |
10+ years | $135,000 - $175,000 | $165,000 - $220,000 | +$30-45K for AGACNP | Both established; AGACNP earning premium |
AGACNP salaries are 8-15% higher nationally, with the gap widening over years of experience. However, AGACNP jobs typically include shift differentials (nights, weekends), overtime pay, and call pay—components of the salary bump. AGPCNP jobs are usually 9-5, Monday-Friday, with rare on-call. Which earning model fits your lifestyle?
Regional Variations: Coastal metropolitan areas (San Francisco, New York, Boston) pay both specialties significantly higher (15-25% above national average) but have high cost of living. Rural areas pay 10-15% below national average but also have lower cost of living. Sunbelt states (Florida, Arizona, Texas) have high demand for both specialties due to aging populations. Midwest and upper Midwest have steady demand but modest salaries.
Exam Content Differences: What You'll Study
The certification exams reflect the scope differences. AANP and ANCC both offer AGPCNP and AGACNP exams, with content tailored to each specialty.
AGPCNP Exam Emphasis (AANP 150 Q, 3 hrs): Assessment and history-taking (35-40%), pharmacology (25-30%), health promotion (15-20%), disease management (15-20%), professional role (5-10%). Heavy emphasis on prevention, chronic disease trajectories, medication management in stable patients, and geriatric assessment. Many questions ask about screening recommendations, deprescribing, and managing multiple chronic diseases simultaneously.
AGACNP Exam Emphasis (AACN 200 Q, 4 hrs): Physiological concepts (20%), health assessment (15%), pharmacology (20%), acute/critical illness (30%), health promotion (5%), professional role (10%). Heavy emphasis on rapid assessment, acute disease protocols, hemodynamic monitoring, ICU pharmacology, and complications. Many questions ask about ventilator management, vasopressor titration, recognizing deterioration, and preventing multi-organ failure.
Study differently for each exam. AGPCNP preparation emphasizes chronic disease guidelines (ADA for diabetes, ACC/AHA for heart disease); AGACNP preparation emphasizes acute illness protocols (sepsis bundles, ARDS management). The knowledge overlaps (both need to know medications), but the application differs fundamentally.
Daily Work: What Your Day Actually Looks Like
AGPCNP Day in a Primary Care Clinic:
8:00 AM: Pre-visit huddle with team. Review chart for Maria, 71, with diabetes and hypertension coming in for routine visit. Note: recent A1C 8.2%. Plan: assess medication adherence, consider increasing metformin, discuss weight loss, order annual labs.
8:30 AM - 12:30 PM: See 12 patients (20-30 min each). Range: annual wellness visits, hypertension follow-up, evaluation of new cough, diabetes management, medication refills, discussions about advance directives. Interrupt: patient with chest discomfort—do EKG, assess, determine need for ED referral.
12:30 PM - 1:15 PM: Lunch (often at desk reviewing labs and returning calls).
1:15 PM - 4:30 PM: See 8-10 more patients. Administrative time: prescription authorizations, prior auth for medications, referral letters to cardiologist or endocrinologist. Review labs from morning visits, adjust medications, call patients with results.
4:30 PM - 5:30 PM: Charting, medication refills, callback time for patients with questions. Prepare visit summaries and send to patients' pharmacies.
Stressors: Patient no-shows, medication insurance denials, complex chronic disease requiring time to counsel and educate, managing difficult medication side effects, addressing social determinants (food insecurity, housing, transportation) that affect health outcomes.
AGACNP Day in a Medical ICU:
6:45 AM: Report from night shift. Census 12 patients. Priorities: 75-year-old with septic shock (vasopressor-dependent), 68-year-old post-op day 2 with acute kidney injury, 79-year-old with acute decompensated heart failure. Night shift: one patient coded (code blue response), post-resuscitation patient on mechanical ventilation.
7:00 AM - 8:00 AM: Rapid bedside assessment of all 12 patients. Vital signs, vent settings, urine output, labs, imaging. Decision: septic shock patient needs higher norepinephrine dose. AKI patient's creatinine is rising—consider starting renal replacement therapy (RRT). HF patient's O2 is dropping—increase PEEP on ventilator.
8:00 AM: Rounds with critical care team (attending, fellows, residents, RNs, respiratory therapy, PT/OT). Present updates on each patient. Order changes: start RRT for AKI patient, wean sedation on post-code patient, change antibiotics based on culture results.
8:00 AM - 12:00 PM: Execute care changes. Titrate vasopressors every 30 minutes based on blood pressure and lactate trends. Monitor new ventilator settings. Communicate with family about code status (patient is declining—discuss goals of care). Place central line in septic shock patient. Respond to acute change: 68-year-old becomes hypoxic—assess lung sounds, review CXR, suspect pneumothorax—call for stat bedside ultrasound.
12:00 PM - 1:00 PM: Lunch (often at bedside if critically ill patient needs monitoring). Calls to specialists (nephrology for RRT orders, cardiology for decompensated HF management).
1:00 PM - 4:00 PM: Continue monitoring, titration, and responding to changes. Patient deteriorating: systemic inflammatory response turning septic—increase vasopressors, contact family, update goals of care. Post-code patient waking up—adjust sedation, assess neurological function, plan for extubation vs. continued mechanical ventilation.
4:00 PM - 5:00 PM: Handoff to night team. Update each patient's story, current vasopressor/ventilator settings, pending labs, anticipated changes overnight. Sign out critical decisions and patient response trends.
Stressors: Patients deteriorating despite your best efforts, moral distress (aggressive care vs. comfort care discussions), shift work and circadian disruption, high cognitive load (12 critically ill patients, each with multiple organ systems failing), family expectations and end-of-life discussions.
These are very different work experiences. Which resonates with you?
Certification Requirements: Which Exam to Take
Both AANP and ANCC offer AGPCNP and AGACNP exams. Most programs prepare you for your chosen specialty, and you sit for the corresponding exam. Switching between specialties after certification requires a new exam (most states don't allow practicing outside your certification, so AGPCNP cert won't let you work as AGACNP without new certification).
AGPCNP Exams: AANP AGPCNP (150 questions, 3 hours, $315) or ANCC AGPCNP (175 questions, 3.5 hours, $395). Both accepted nationally. Similar pass rates (AANP 87%, ANCC 80%). Choose based on question style preference and program recommendation.
AGACNP Exams: AACN AGACNP (200 questions, 4 hours, $395) is the primary option. AANP does not offer AGACNP exam (AANP focuses on primary care specialties). AACN is the dominant AGACNP certifier. Pass rate ~82%.
This is an important distinction: if you choose AGACNP, you must sit for AACN. If you choose AGPCNP, you can choose between AANP and ANCC (most choose AANP for lower cost and slightly higher pass rate). Both primary care exams are accepted in all 50 states for licensure.
Career Trajectory: Where Each Path Leads
AGPCNP Career Progression: New grad → Primary care clinician → Lead clinician or project manager → Geriatric specialist or program director → Faculty/educator. Many AGPCNPs transition to education, quality improvement, or administration after 8-12 years. Some pursue doctoral research in geriatrics. Others become specialists in specific areas (palliative care, gerontology, women's health in older adults). The trajectory is flexible—you can shift between direct care and leadership roles.
AGACNP Career Progression: New grad → ICU clinician → Charge nurse (leadership role in ICU) → Clinical educator or quality improvement specialist → ICU director or system-level leadership. Most AGACNPs stay in direct care longer than AGPCNPs (8-15 years average before transition). Some become critical care specialists or pursue critical care research. Fewer transition to non-bedside roles early in career—ICU culture emphasizes clinical expertise.
If you see yourself eventually leaving direct patient care for leadership, education, or research, AGPCNP offers faster transition. If you're passionate about critical care and want to remain clinically active long-term, AGACNP suits you.
Decision Framework: Which Specialty Is Right for You?
Choose AGPCNP if: You enjoy longitudinal relationships with patients and their families. You prefer structured, scheduled work with predictable days. You want flexibility to work in diverse settings (clinic, telehealth, nursing home, urgent care). You're interested in chronic disease management, prevention, and health promotion. You value geographic flexibility and geographic arbitrage (rural = lower living costs + good salary). You see yourself eventually transitioning to leadership, education, or research. You prefer stable work-life balance and predictable off-hours availability.
Choose AGACNP if: You thrive in fast-paced, high-acuity environments. You enjoy rapid decision-making and seeing immediate results of your interventions. You're drawn to the intensity and complexity of critical illness. You're comfortable with shift work and on-call responsibilities. You prefer higher salary compensation. You're willing to work primarily in hospitals and accept geographic concentration of jobs. You're passionate about critical care and want to build deep expertise in ICU medicine. You see yourself staying in direct patient care long-term.
Pro Tip: Before committing, shadow an AGPCNP in a primary care clinic and an AGACNP in an ICU for a full shift each. You'll quickly discover which environment energizes you and which drains you. That visceral reaction matters more than any career analysis.
Program Selection: What to Look For
Your graduate program determines your certification path. Most programs offer one specialty (AGPCNP or AGACNP); some offer both tracks. If you're undecided, choose a program that offers flexibility or allows specialization in year 2.
AGPCNP Program Indicators: Faculty with primary care backgrounds. Clinical rotations in outpatient clinics, nursing homes, urgent care. Emphasis on chronic disease management, health promotion, and evidence-based primary care guidelines. Strong connections to community health centers and rural clinics.
AGACNP Program Indicators: Faculty with ICU/critical care backgrounds. Clinical rotations in ICUs (medical, surgical, or mixed). Emphasis on acute illness protocols, hemodynamic monitoring, and critical care guidelines. Strong connections to major health systems with robust ICU programs.
Talk to current students in each program. Ask: "What is the job market like for graduates?" "Where do alumni work?" "What is the pass rate on board exam?" "How much do you feel prepared for your chosen specialty?" These conversations matter more than rankings.
Keep Reading: Deepen Your AGNP Knowledge
Strengthen your understanding of AGNP specialization and exam preparation:
The Ultimate AGNP Exam Study Guide for 2026: Master the 12-week study timeline, domain weightings, and 2,000-question strategy that gets students to exam-ready competency. https://hltmastery.com/nursing/agnp/resources/agnp-exam-study-guide-2026
Why AGNP Students Struggle: Learn the 5 most common challenges students face and evidence-based solutions to overcome them. https://hltmastery.com/nursing/agnp/resources/why-agnp-students-struggle
AGNP Pharmacology: Geriatric Drug Review: Master Beers Criteria, age-related pharmacokinetic changes, and high-yield drug interactions essential for both specialties. https://hltmastery.com/nursing/agnp/resources/agnp-pharmacology-geriatric-drug-review
AANP vs ANCC for AGNP: Compare the two major exam boards, their content differences, pass rates, and exam-specific study strategies. https://hltmastery.com/nursing/agnp/resources/aanp-vs-ancc-for-agnp-which-exam
Final Word
AGPCNP and AGACNP are both critical nursing roles. The choice between them is not about status or prestige—they're equally important to the healthcare system. The choice is about which environment and patient population you'll be most effective in, which work schedule suits your life, and which career trajectory excites you.
Talk to practicing AGPCNPs and AGACNPs. Shadow both specialties. Reflect on what energizes you: Is it the long-term relationship with a patient managing diabetes, or the acute crisis where you save a septic patient's life? Is it the quiet continuity of primary care, or the intensity of the ICU?
The right choice is the one that makes you wake up excited to go to work. Choose that, and you'll be excellent at it.
Ready to specialize? HLT Mastery has guided over 400,000 nurses through specialization decisions and board exam preparation. Whether you're pursuing AGPCNP or AGACNP, we have specialty-specific study plans, expert content, and a community of nurses preparing for the same certification. Join our AGNP program today—let's get you certified and confident in your specialty.
NCLEX Mastery
\
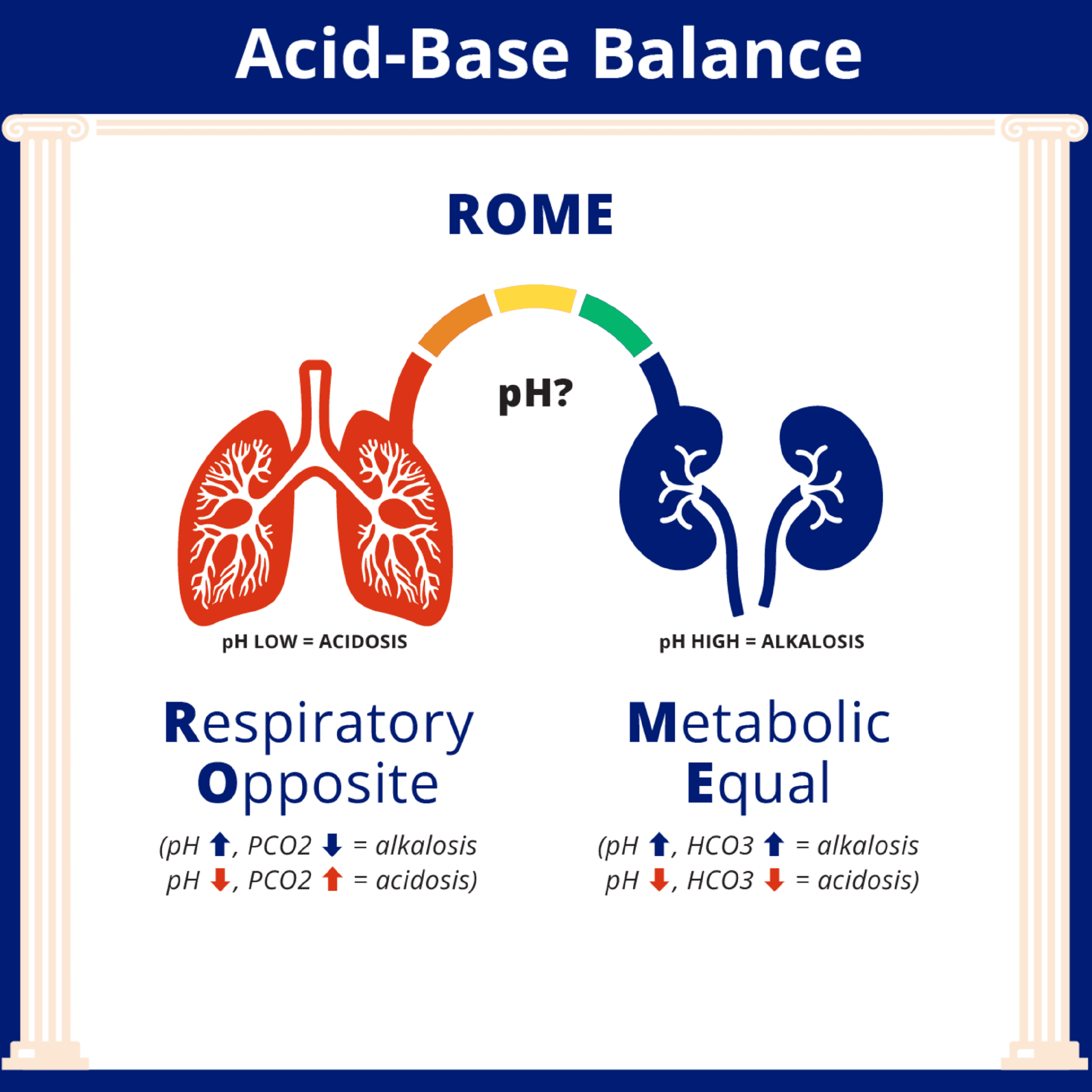
How to Interpret ABGs for the NCLEX
How to Interpret ABGs for the NCLEX

NCLEX Mastery
\
Estimating TBSA: What Every Nurse Should Know
Estimating TBSA: What Every Nurse Should Know

Catherine Cantrell, MSN, RN
\
What Actually Happens When You Fail a Nursing Course




