Kristin Everhart, MSN, ARNP, FNP-C
\
Apr 7, 2026

You're reviewing a patient's medication list: lisinopril, hydrochlorothiazide, metoprolol, amlodipine, metformin, ibuprofen (600 mg three times daily), diphenhydramine (for sleep), and omeprazole. The patient is an 81-year-old woman with hypertension, type 2 diabetes, and arthritis. She's been on this regimen for 2 years, and her family says she's "more forgetful lately" and "has fallen twice in the past month." You recognize immediately that her medication list is a problem. The ibuprofen is contraindicated with her diuretic and ACE inhibitor (cardiorenal syndrome risk). The diphenhydramine is causing her confusion and falls. She's on four blood pressure medications when her systolic is 110—over-treated. But do you know what to deprescribe and what to add in place? If you're not confident, you're not alone. Pharmacology is the #1 area where AGNP students struggle, with a 42% incorrect-answer rate across all test-takers on the 2024-25 exams.
This guide is a high-yield review of geriatric pharmacology for the AGNP exam. We've broken down Beers Criteria into actionable tables, mapped age-related pharmacokinetic changes to clinical decisions, created decision frameworks for deprescribing, and provided deep dives on high-yield drug classes. By the end, you won't just know drug names. You'll understand how a 78-year-old's body processes medication differently than a 45-year-old's, and how to prescribe and deprescribe accordingly.
Key Insight: Geriatric pharmacology is not about memorization. It's about understanding two principles: (1) Age changes how the body processes drugs (pharmacokinetics), and (2) Aging changes how drugs work in the body (pharmacodynamics). Master these two principles, apply them to Beers Criteria and common drug classes, and you'll pass pharmacology questions reliably. Memorize drug names without understanding principles, and you'll fail when the question tests an unfamiliar drug.
Age-Related Pharmacokinetic Changes: Why Elderly Process Drugs Differently
A 40-year-old takes 500 mg of metformin twice daily for diabetes; it clears from his body through his kidneys. An 81-year-old takes the same dose, but his glomerular filtration rate (GFR) is 40 (down from normal 100+). The metformin accumulates in his bloodstream, increasing his risk of lactic acidosis. Same drug, same dose, different body—different consequence. This is pharmacokinetics: how the body absorbs, distributes, metabolizes, and excretes drug.
Absorption (GI Tract → Bloodstream):
Changes with age: Reduced gastric acid (higher pH), slower gastric emptying, decreased GI blood flow, reduced intestinal surface area.
Clinical consequences: Some drugs absorb slower (delayed onset of action). Some drugs absorb unpredictably (wide variation in blood levels between patients). Some drugs don't absorb well at all (low bioavailability).
Practical examples:
- Digoxin: Reduced stomach acid decreases absorption by 20-30% in elderly. If an 82-year-old is on chronic digoxin at a dose appropriate for a 50-year-old, his digoxin level will be subtherapeutic. Add omeprazole for GERD (further reducing acid), and absorption drops even more. Solution: Check digoxin levels; adjust dose based on levels, not age alone.
- Calcium supplements: Must be taken with food and adequate stomach acid. In elderly on PPIs, calcium absorption plummets. Solution: Use calcium citrate (absorbs better at low pH) instead of calcium carbonate, or consider alternative osteoporosis therapy.
- Alendronate (bisphosphonate): Requires specific dosing (30-60 min before food, with 8 oz water, upright position). In elderly with slow GI motility and who forget instructions, absorption is minimal. Often ineffective. Solution: Consider IV zoledronic acid for improved bioavailability.
Distribution (Bloodstream → Tissues → Action Site):
Changes with age: Increased body fat (18% at age 20 → 30% at age 70), decreased total body water, decreased serum albumin, increased alpha-1 acid glycoprotein.
Clinical consequences: Lipophilic (fat-soluble) drugs accumulate in fat, increasing half-life and risk of toxicity. Water-soluble drugs concentrate higher in serum. Drugs that bind to albumin become more active (less protein binding → higher free drug → more active).
Practical examples:
- Benzodiazepines (lipophilic): Diazepam half-life is 20-30 hours in younger adults, 50-100+ hours in elderly due to fat accumulation. Long-acting benzos accumulate over weeks, causing prolonged sedation, falls, and cognitive impairment. Solution: Avoid long-acting benzos in elderly. If needed, use short-acting agents (lorazepam, oxazepam, temazepam) at reduced doses.
- Warfarin (highly protein-bound): Decreased albumin in elderly means more free, active warfarin. INR increases without dose change. Solution: Start warfarin at lower doses in elderly; check INR frequently; educate on consistency of vitamin K intake.
- Digoxin: Narrow therapeutic window; decreased volume of distribution in elderly means higher serum levels at standard dose. Solution: Use lower doses; check levels at steady state (5-7 days).
- Propranolol (lipophilic): Accumulates in fat. Higher doses needed initially, but effects plateau unexpectedly over weeks as accumulation catches up. Solution: Start low, go slow; give weeks to assess effect before increasing.
Metabolism (Liver → Inactivated/Active Drug):
Changes with age: Reduced hepatic blood flow (25-40% decrease at age 80), decreased CYP450 enzyme activity, reduced phase II metabolism (conjugation).
Clinical consequences: Drugs metabolized by liver are cleared more slowly. Prodrugs (inactive drugs converted to active metabolites by CYP450) become less effective. Active metabolites accumulate.
Practical examples:
- Codeine (prodrug activated by CYP2D6): Effectiveness depends on conversion to morphine. In elderly with reduced CYP2D6 activity, codeine is less effective. Some patients also have genetic CYP2D6 variants, making them "poor metabolizers" of codeine. Solution: Use immediate-release morphine instead of codeine for elderly; predictable effect, no metabolite dependence.
- Midazolam (sedative metabolized by CYP3A4): Elderly have reduced CYP3A4. Standard dose causes prolonged sedation. Solution: Reduce dose by 25-50% in elderly; use for acute anxiety, not chronic; monitor for oversedation.
- Theophylline (metabolized by CYP1A2, CYP3A4): Clearance decreases by 30-40% in elderly. Narrow therapeutic window. Small dose increases can push serum level into toxic range. Solution: Rarely used now (replaced by albuterol); if used, check levels.
- Atorvastatin (hepatic metabolism): Elderly have reduced metabolism. Higher steady-state levels, risk of myopathy. Solution: Use lower starting doses; monitor CK; consider pravastatin (not metabolized) as alternative.
Excretion (Kidneys → Urine or Hepatic Clearance):
Changes with age: GFR declines ~1 mL/min/year after age 30. By age 80, GFR may be 40-50 (normal ~90-120). BUT serum creatinine can be normal because muscle mass also declines. Never use serum creatinine alone to assess renal function in elderly.
Clinical consequences: Renally cleared drugs accumulate. Electrolyte abnormalities occur more easily. Nephrotoxic drugs (NSAIDs, ACE inhibitors in certain settings, aminoglycosides, contrast dye) cause acute kidney injury more readily.
Practical examples:
- Metformin: Excreted unchanged in urine. Contraindicated if eGFR <30 due to lactic acidosis risk. Solution: Calculate eGFR using CKD-EPI (accounts for age and muscle mass). Don't rely on serum creatinine. Reduce metformin dose if eGFR 30-45.
- Digoxin: Cleared by kidneys. Elderly with eGFR <40 accumulate digoxin rapidly. Toxic levels within days. Solution: Use lower doses; space out doses; check levels; consider alternatives (beta-blockers for rate control instead of digoxin).
- Lisinopril (ACE inhibitor): Cleared by kidneys. Accumulates in renal disease. Can cause hyperkalemia + acute kidney injury (especially with NSAIDs and potassium-sparing diuretics). Solution: Check renal function before starting; monitor K+ and creatinine after dose changes; educate on NSAID avoidance.
- Morphine (opioid): Metabolized to morphine-3-glucuronide and morphine-6-glucuronide (both active), excreted by kidneys. In renal disease, metabolites accumulate, causing prolonged respiratory depression. Solution: Use lower doses; longer intervals between doses; monitor closely.
- Aminoglycosides (antibiotics): Nephrotoxic; cleared by kidneys. Accumulation in elderly with renal impairment causes acute kidney injury. Solution: Avoid if possible; if necessary, use once-daily dosing (reduces nephrotoxicity) and check trough levels; monitor creatinine daily; hydrate well.
Beers Criteria: Drugs to Avoid or Use With Extreme Caution in Elderly (65+)
The American Geriatrics Society Beers Criteria (updated 2023) lists medications to avoid in adults 65+ due to high risk of adverse effects, particularly in those with polypharmacy. Know these categories cold—they're heavily tested.
Drug Class | Specific Examples | Why Avoid in Elderly (Age 65+) | Adverse Effects | Better Alternative |
|---|---|---|---|---|
Benzodiazepines (AVOID) | Diazepam, lorazepam, alprazolam, clonazepam; all durations problematic | Increased risk of cognitive impairment, delirium, falls, fractures, motor vehicle crashes; addiction risk even at low doses; withdrawal risk | Confusion, oversedation, ataxia, falls, hip fractures (20-50% increase) | SSRI (sertraline, paroxetine) for anxiety; melatonin 1-5 mg for sleep; buspirone for anxiety |
Anticholinergics (AVOID) | Diphenhydramine, hydroxyzine, promethazine, benztropine, dicyclomine, scopolamine | Strongly anticholinergic; potent cognition/delirium risk; increased falls, constipation, urinary retention | Confusion, delirium, urinary retention, severe constipation, blurred vision, tachycardia, falls | For allergies: non-sedating antihistamines (cetirizine, loratadine). For sleep: melatonin, trazodone (low-dose). For nausea: domperidone or ginger |
NSAIDs (Chronic Use) (CAUTION) | Ibuprofen, naproxen, indomethacin; NOT aspirin or topical NSAIDs | GI bleed risk (especially with anticoagulants/antiplatelets); acute kidney injury; hyperkalemia; HTN worsening | GI bleed, acute kidney injury, hyperkalemia, elevated BP, medication interactions | Acetaminophen (up to 3g/day if normal liver function). Topical diclofenac or capsaicin. Physical therapy. Low-dose opioids for severe pain |
Meperidine (AVOID) | Demerol (opioid analgesic) | Active metabolite normeperidine is neurotoxic; accumulates in renal disease; causes tremor, confusion, seizures | Neurotoxicity (tremor, confusion, hallucinations), seizures if renal dysfunction | Morphine or hydromorphone (no neurotoxic metabolites) |
Sedating Tricyclic Antidepressants (CAUTION) | Amitriptyline, doxepin, imipramine (tertiary amines) | Anticholinergic effects, orthostatic hypotension, sedation, confusion, falls | Confusion, falls, orthostasis, constipation, urinary retention | SSRI (sertraline, paroxetine) or SNRI (duloxetine for pain/depression combo). For neuropathic pain: gabapentin or pregabalin |
Fluoxetine & Long-Acting SSRIs (CAUTION) | Fluoxetine (long half-life ~50-70 hrs); paroxetine (high anticholinergic) | Long half-life causes drug interactions, withdrawal symptoms; paroxetine has anticholinergic effects | Drug interactions, withdrawal, confusion (paroxetine) | Sertraline or citalopram (shorter half-life, fewer interactions; citalopram limited to 20 mg/day in 60+ due to QT prolongation) |
Sulfonylureas (Older Agents) (CAUTION) | Glyburide, glipizide (high hypoglycemia risk) | High hypoglycemia risk; elderly have blunted hypoglycemia symptoms (no tremor/diaphoresis); confusion/falls from hypoglycemia | Severe hypoglycemia, confusion, falls, seizures | Metformin, GLP-1 agonist (semaglutide), DPP-4 inhibitor (sitagliptin), SGLT-2 inhibitor; if needed, low-dose glipizide |
Thiazolidinediones (CAUTION) | Pioglitazone, rosiglitazone | Volume expansion, worsening heart failure, bone loss/increased fracture risk, fluid retention | Heart failure exacerbation, ankle edema, fractures | GLP-1 agonist, SGLT-2 inhibitor, or lower-dose insulin |
Estrogens (AVOID) | Conjugated estrogens, estradiol | Increased risk of breast cancer, clot, stroke; minimal bone benefit after age 70; unnecessary in most | DVT, PE, stroke, breast cancer | Avoid if >65. For hot flashes: SSRI (paroxetine, venlafaxine). For vaginal dryness: vaginal estrogen (localized, minimal absorption) |
Proton Pump Inhibitors (PPIs) (CAUTION - chronic use) | Omeprazole, lansoprazole, pantoprazole (long-term use) | Increased fracture risk; B12/magnesium deficiency; increased infection risk (C. difficile); may interfere with other drug absorption | Fractures, B12 deficiency (megaloblastic anemia), hypomagnesemia, infections | H2 blocker (famotidine) for episodic reflux. Deprescribe if on >8 weeks and no ongoing indication. Taper slowly |
Anticholinergic Burden (Cumulative) (AVOID combinations) | Any combo of diphenhydramine + benztropine + dicyclomine + tricyclic antidepressant + anticholinergic antiemetic | Cumulative anticholinergic effect → severe confusion, urinary retention, constipation; effects multiply, not add | Delirium, urinary retention, fecal impaction, falls | Review entire medication list; deprescribe high-anticholinergic drugs systematically |
How to Use Beers Criteria on the Exam: When you see a medication list, scan for Beers drugs first. If a patient is on benzodiazepine + anticholinergic + NSAID, their symptoms of confusion and falls are likely medication-induced. The question might ask "Which medication should be deprescribed?" and the answer is often "Stop the benzodiazepine." Don't overthink—identify the Beers drug and remove it (or justify why it's an exception).
START/STOPP Criteria: Beyond Beers—The European Approach
Beers Criteria is American; START/STOPP is European. START = drugs that Should be considered in older people for certain conditions (explicit deprescribing targets). STOPP = drugs that Significantly increase adverse effects. Some exam questions use START/STOPP language. Know the concept: START identifies undertreatment (patients on too few medications); STOPP identifies overtreatment (patients on contraindicated drugs).
Key START Examples (Often Tested):
- Patient with heart failure should be on ACE inhibitor (if EF <40%)? YES, START drug.
- Patient with AF should be on anticoagulant (CHADS2-VASc ≥1)? YES, START drug.
- Patient with osteoporosis should be on bisphosphonate? YES, START drug (if not high fracture risk).
- Patient with depression should be on antidepressant? YES, START drug.
These are often paired with STOPP (stop something bad) to test whether you can deprescribe and prescribe simultaneously. Example: "82-year-old on benzodiazepam for anxiety AND (should be on) SSRI for anxiety. What's your plan?" Answer: STOP benzodiazepam, START SSRI, taper benzo slowly to avoid withdrawal.
High-Yield Drug Classes for the AGNP Exam
Rather than memorizing every drug, master the drug classes most tested and most high-yield for geriatric patients.
Antihypertensives in Elderly: Target BP Changes With Age
ACE Inhibitors (lisinopril, enalapril, ramipril): First-line for HTN + diabetes or HF. Monitor K+ (hyperkalemia risk). Check creatinine after initiation (can transiently increase 20-30%, usually self-limited). Avoid in pregnancy (not relevant for AGNP) and renal artery stenosis.
ARBs (losartan, valsartan, olmesartan): Equivalent to ACE-I in elderly; slight lower cough risk. Same monitoring (K+, creatinine). Use if ACE-I intolerant.
Thiazide Diuretics (HCTZ, chlorthalidone): Second-line; beware hypokalemia, hyponatremia, gout flare in elderly. Chlorthalidone is more potent than HCTZ (longer half-life, 12.5 mg = 50 mg HCTZ). Elderly on thiazide need baseline K+ check, then recheck in 2 weeks and 1-2 months.
Beta-Blockers (metoprolol, atenolol, carvedilol): Excellent if post-MI or HF; avoid monotherapy for HTN alone (doesn't reduce MI/stroke as effectively as other agents). Slow heart rate can worsen depression and fatigue in elderly. Beware bradycardia and hypotension. Cardioselective agents (metoprolol, atenolol) better than non-selective (propranolol).
Calcium Channel Blockers (amlodipine, nifedipine ER, diltiazem): Excellent agents; amlodipine (long-acting dihydropyridine) preferred. Beware ankle edema (not heart failure, just drug effect). Diltiazem/verapamil non-dihydropyridines can worsen bradycardia/hypotension; avoid if baseline HR <60 or SBP <110.
BP Target by Age (Geriatric-Specific):
- Age 65-75, no prior stroke: Target SBP 130-140 (not <130; increases fall risk).
- Age 75-85: Target SBP 140-150 (tight control increases syncope/falls).
- Age 85+: Target SBP 140-160 (deprioritize antihypertensives if causing orthostasis).
- Prior stroke: Maintain SBP 130-150 (ultra-tight control <130 may worsen stroke recurrence by reducing cerebral perfusion).
Exam question: "82-year-old with prior stroke on lisinopril, HCTZ, metoprolol, amlodipine. SBP 115. Recent syncope. Plan?" Answer: DEPRESCRIBE one BP medication (likely HCTZ—easiest to stop). Target SBP 130-150.
Diabetes Management in Elderly (75+): De-Intensify Glycemic Control
Metformin (first-line): Safe if eGFR >30. Check eGFR at baseline and annually. Reduce dose if eGFR 30-45. No renal dose available; either full dose or contraindicated. Hold if contrast dye (lactic acidosis risk from iodine + metformin + renal dysfunction). Restart 48 hrs after contrast if renal function stable.
GLP-1 Agonists (semaglutide, liraglutide): Excellent in elderly; weight-neutral or weight-loss. Cardiovascular benefit + renal protection. GI side effects (nausea) main limiting factor in elderly. Injectable weekly (semaglutide) easier than daily injections. Starting dose must be low to minimize nausea.
SGLT-2 Inhibitors (empagliflozin, canagliflozin): Excellent in elderly especially with HF or CKD. Cardiovascular and renal protective. Beware euglycemic DKA (rare but serious; occurs at normal glucose). Genitourinary infections increased (~10% absolute increase). Monitor for volume depletion in summer heat.
DPP-4 Inhibitors (sitagliptin, saxagliptin): Very safe, modest glucose lowering. Good for elderly with minimal side effects. No hypoglycemia risk. Reduce dose if eGFR <30.
Sulfonylureas (glyburide, glipizide) & Meglitinides (repaglinide): HIGH HYPOGLYCEMIA RISK. Elderly have blunted hypoglycemia symptoms (no tremor/diaphoresis); confusion/falls are only sign. Avoid or use extreme caution. If needed, glipizide (shorter-acting) preferred to glyburide. Use lowest dose.
Insulin: Necessary in T1DM; in T2DM, defer until other agents fail. High hypoglycemia risk in elderly. If starting, use long-acting basal insulin (glargine or detemir) at low dose; titrate slowly. Teach patient/caregiver recognition of hypoglycemia and glucagon use.
A1C Target by Age and Comorbidity (Geriatric-Specific):
- Age <75, no major comorbidity: A1C 7% (standard).
- Age 75-85, or multiple comorbidities: A1C 7-8% (less aggressive).
- Age 85+, or advanced comorbidity/dementia: A1C 8-9% (focus on avoiding hypoglycemia).
- Life expectancy <5 years: Deprioritize diabetes control; focus on comfort.
Exam question: "78-year-old with HF, CKD stage 3, A1C 8.5% on metformin and SGLT-2i. On glyburide. Recent hypoglycemic episode. Plan?" Answer: STOP glyburide (high hypoglycemia risk). Continue metformin + SGLT-2i. A1C 8-8.5% is acceptable target for this age/comorbidity. No intensification needed.
Anticoagulation in Atrial Fibrillation (Elderly at Highest Stroke Risk)
Direct Oral Anticoagulants (DOACs): Apixaban, dabigatran, edoxaban, rivaroxaban. Preferred over warfarin in elderly because no INR monitoring, fewer drug interactions, predictable pharmacokinetics. Dosing reduced by age/weight/renal function. Apixaban least renal clearance (safest in advanced CKD). Dabigatran highest bleed risk. Edoxaban highest bleed risk if weight <50 kg.
Warfarin: Effective but requires INR monitoring; many drug interactions; higher bleeding risk if INR subtherapeutic then over-corrected. Use ONLY if DOAC contraindicated (e.g., mechanical heart valve, severe hepatic disease, allergy). Target INR 2-3 for AFib.
Antiplatelet Monotherapy (Aspirin 81 mg): NO LONGER RECOMMENDED for stroke prevention in AFib. Only use if patient refuses anticoagulation and very low stroke risk (CHA2DS2-VASc 0-1 in men, 0-2 in women).
Anticoagulation Decision in Elderly AFib (Common Exam Question):
78-year-old woman, AFib x3 months, HTN, DM, prior stroke (CHA2DS2-VASc = 5). eGFR 35. "Do you start anticoagulation?" Answer: YES, high stroke risk. Which agent? Apixaban (least renal clearance, safest with eGFR 35). Warfarin also acceptable if DOAC contraindicated, but DOAC preferred. Question tests both decision to anticoagulate and selection of safest agent for this patient's renal function.
Bone Health: Osteoporosis Medications in Elderly
Bisphosphonates (alendronate, risedronate, zoledronic acid): First-line for osteoporosis prevention. Weekly or monthly oral (alendronate/risedronate) or yearly IV (zoledronic acid). CRITICAL: Alendronate/risedronate require specific dosing (30-60 min before food, 8 oz water, sit upright 30 min). Elderly often forget or do wrong → no absorption → ineffective. IV zoledronic acid bypasses absorption; preferred for cognitively impaired. Beware jawbone necrosis and atypical fractures with long-term use (>5 years); reassess need periodically.
Calcium + Vitamin D: Universal recommendation but evidence weak for fracture prevention if diet adequate. Excessive supplementation increases kidney stones and CVD risk. Target dietary calcium 1000-1200 mg/day; supplement if <800 mg/day. Vitamin D 1000 IU daily or 50,000 IU weekly (if deficient).
Denosumab (monoclonal antibody): Effective for osteoporosis; reduces fracture risk 60-70%. Subcutaneous injection every 6 months. Used when bisphosphonate intolerant or ineffective. High cost; reimbursement often requires bisphosphonate failure first.
Pain Management in Elderly: Avoid Opioids, Optimize Alternatives
Acetaminophen: Up to 3-4 g/day if normal liver function (but many elderly on 500-1000 mg doses prescribed by multiple providers—educate on total daily limit). Safer than NSAIDs. No interaction with anticoagulants. More effective than opioids for mild-moderate pain in many elderly.
Topical NSAIDs (diclofenac cream/patch): Excellent for localized pain (arthritis, muscle strain). Minimal systemic absorption. Low bleed risk. Preferred over oral NSAIDs in elderly.
Neuropathic Pain Agents (gabapentin, pregabalin, duloxetine): For neuropathic pain (diabetic neuropathy, post-herpetic neuralgia, fibromyalgia). Start low, titrate slowly. Gabapentin 300 mg TID is standard; reduce dose if eGFR <30. Pregabalin also requires dose adjustment. Duloxetine (SNRI) 30-60 mg daily; also treats depression if co-existing.
Opioids (morphine, hydromorphone): RESERVE for cancer pain, end-of-life care, or pain unresponsive to above. In elderly, use lowest dose, longest interval (e.g., morphine 5 mg every 6-8 hrs, not 15 mg). High overdose risk. Teach caregiver to recognize respiratory depression. Beware opioid-induced constipation (almost universal in elderly); start bowel regimen concurrently (stool softener + osmotic laxative).
Avoid in Elderly with Chronic Pain: NSAIDs (GI bleed/AKI/hyperkalemia risk), meperidine (neurotoxic metabolites), tramadol (seizure risk if dose >300 mg/day or concurrent SSRIs).
Deprescribing Framework: When and How to Stop Medications
Deprescribing is a systematic approach to removing unnecessary or harmful medications. It's as important as prescribing on the AGNP exam.
Five Questions to Ask About Every Medication:
Is the indication still relevant? Patient on omeprazole for GERD diagnosed 5 years ago, but hasn't had reflux in years? Indication no longer relevant → STOP (or trial off to see if symptoms recur).
Is the dose appropriate for age/renal function? Patient on lisinopril 20 mg with eGFR 25? Dose too high → REDUCE (standard dose for eGFR <30 is 5-10 mg).
Are there drug-drug interactions causing harm? Patient on lisinopril + HCTZ + NSAID? Triple threat for hyperkalemia and AKI → STOP NSAID, add alternative pain control.
Is the benefit greater than risk in this patient? 88-year-old with life expectancy 4 years on statin? Benefit of MI prevention over 4 years is minimal (<1 MACE prevented per 100 patients). Continue only if already established for CAD; don't start new.
Are there Beers Criteria concerns? Patient on diphenhydramine for sleep? Beers: AVOID. Replace with melatonin or trazodone.
Deprescribing Steps:
1. Identify medication(s) to deprescribe.
2. Slow taper where needed (especially benzodiazepines—never stop abruptly; withdrawal risk). Example: Alprazolam 0.5 mg TID → 0.5 mg BID x 1 week → 0.5 mg daily x 1 week → 0.25 mg daily x 1 week → STOP.
3. Monitor for withdrawal symptoms or relapse of original condition (e.g., anxiety returning after benzo withdrawal).
4. Reassure patient/family: "We're removing a medication that's causing confusion/falls. You'll likely feel better."
5. Document: why deprescribed, tapering plan, monitoring plan.
Exam question: "82-year-old on 4 BP meds (SBP 110), on diphenhydramine (confusion, falls), on chronic NSAIDs (eGFR 35, hyperkalemia 5.5). Which should you deprescribe first?" Answer: Stop NSAID immediately (dangerous combo with CKD and ACE-I). Taper benzodiazepine/diphenhydramine. Reduce one BP medication. This patient has too many medications causing iatrogenic disease.
Keep Reading: Strengthen Your AGNP Foundation
The Ultimate AGNP Exam Study Guide for 2026: Master the 12-week study timeline; pharmacology is 25-30% of exam weight—make it your priority. https://hltmastery.com/nursing/agnp/resources/agnp-exam-study-guide-2026
Why AGNP Students Struggle: Polypharmacy is Challenge #1. Deep dive into the challenges and solutions. https://hltmastery.com/nursing/agnp/resources/why-agnp-students-struggle
AGPCNP vs AGACNP: Choosing Your Specialty: Pharmacology knowledge differs between primary care (chronic disease) and acute care (ICU drug protocols). Understand your specialty's focus. https://hltmastery.com/nursing/agnp/resources/agpcnp-vs-agacnp-choosing-your-specialty
AANP vs ANCC for AGNP: Both exams test pharmacology heavily; study approach and question format differ. https://hltmastery.com/nursing/agnp/resources/aanp-vs-ancc-for-agnp-which-exam
Final Word: Pharmacology Is Learnable
Pharmacology feels overwhelming because there are thousands of drugs. But the AGNP exam tests principles, not memorization. Master these five principles:
Age changes pharmacokinetics: Absorption, distribution, metabolism, excretion all slow or change with age → drugs stay in body longer → toxicity risk.
Beers Criteria are your roadmap: Know these drugs by heart. When you see them, think "avoid." When you see them causing symptoms, think "deprescribe."
Drug-drug interactions kill elderly: ACE-I + K+-sparing diuretic + NSAID = hyperkalemia + AKI. Memorize the deadly combinations.
Deprescribing is as important as prescribing: Too many medications is a disease. Recognize polypharmacy as a problem. Remove harm before adding treatment.
Life expectancy drives decisions: A treatment that benefits a 65-year-old (30-year life expectancy) may not benefit an 85-year-old (6-year life expectancy). Always ask: "Will this patient live long enough to see benefit?"
You've got this. Pharmacology is the hardest domain for AGNP students, but it's also the most learnable. Dedicate 30% of your study time to pharmacology questions (minimum 300 in this domain alone). By exam day, you'll be comfortable recognizing drug interactions, identifying Beers drugs, and making deprescribing decisions.
Pharmacology mastery starts here: HLT Mastery's AGNP program includes deep pharmacology modules with 500+ practice questions focused on Beers Criteria, polypharmacy, and deprescribing. 27M nurses reached. 2B+ questions answered. 400K+ users this year. Join now—master pharmacology and pass your AGNP exam with confidence.
NCLEX Mastery
\
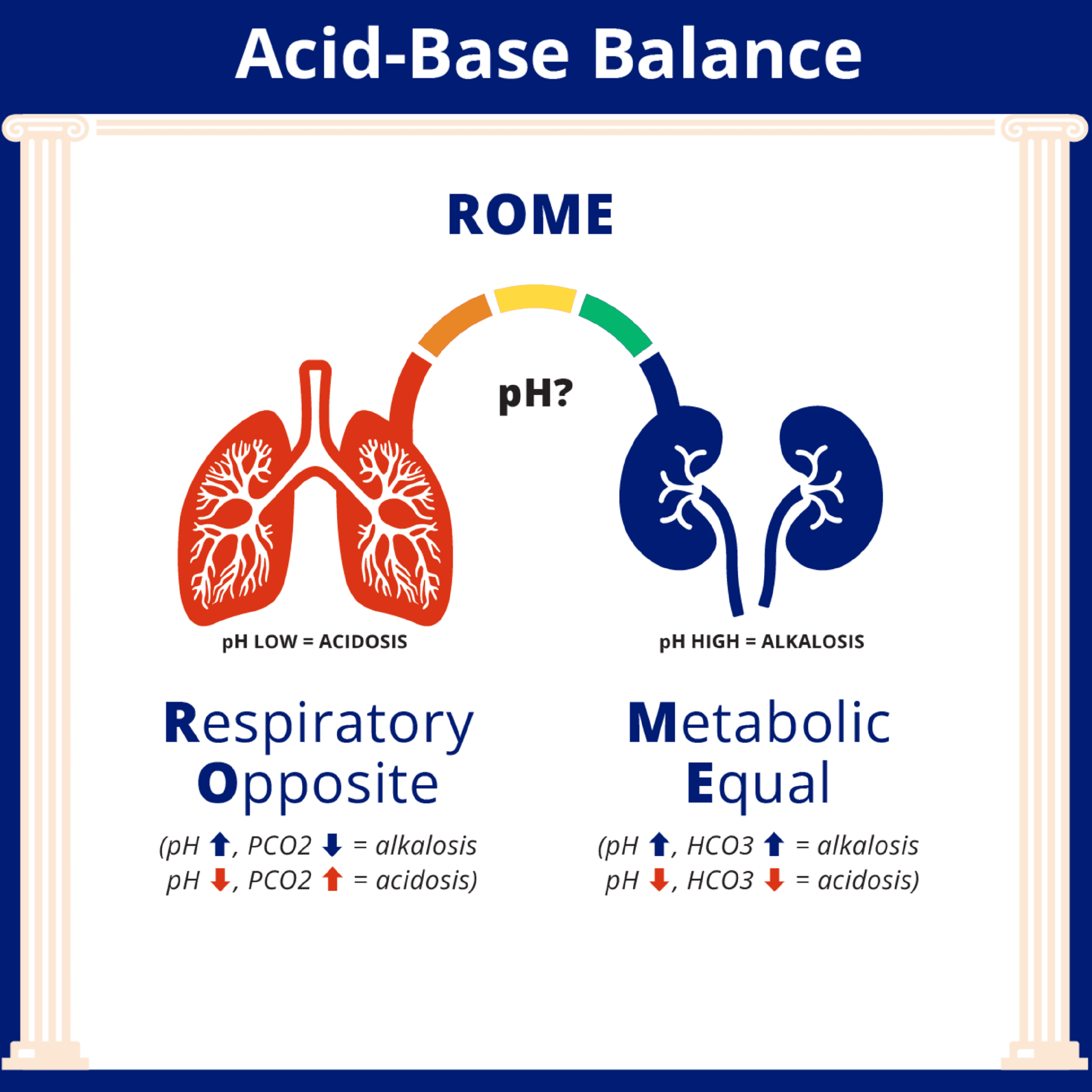
How to Interpret ABGs for the NCLEX
How to Interpret ABGs for the NCLEX

NCLEX Mastery
\
Estimating TBSA: What Every Nurse Should Know
Estimating TBSA: What Every Nurse Should Know

Catherine Cantrell, MSN, RN
\
What Actually Happens When You Fail a Nursing Course




