
NCLEX Mastery
\
Apr 27, 2026
"ABGs make no sense. I've read it five times"
"I know the mnemonic but when I see the actual numbers on a question I freeze"
"I always mix up respiratory and metabolic. Someone explain it like I'm five"
"Compensated vs uncompensated is where I always go wrong"
Sound like you? Well then, READ ON!
Your body works constantly to keep the blood within a narrow, life-sustaining range. When everything is working the way it should, arterial blood gas (ABG) values look like this:
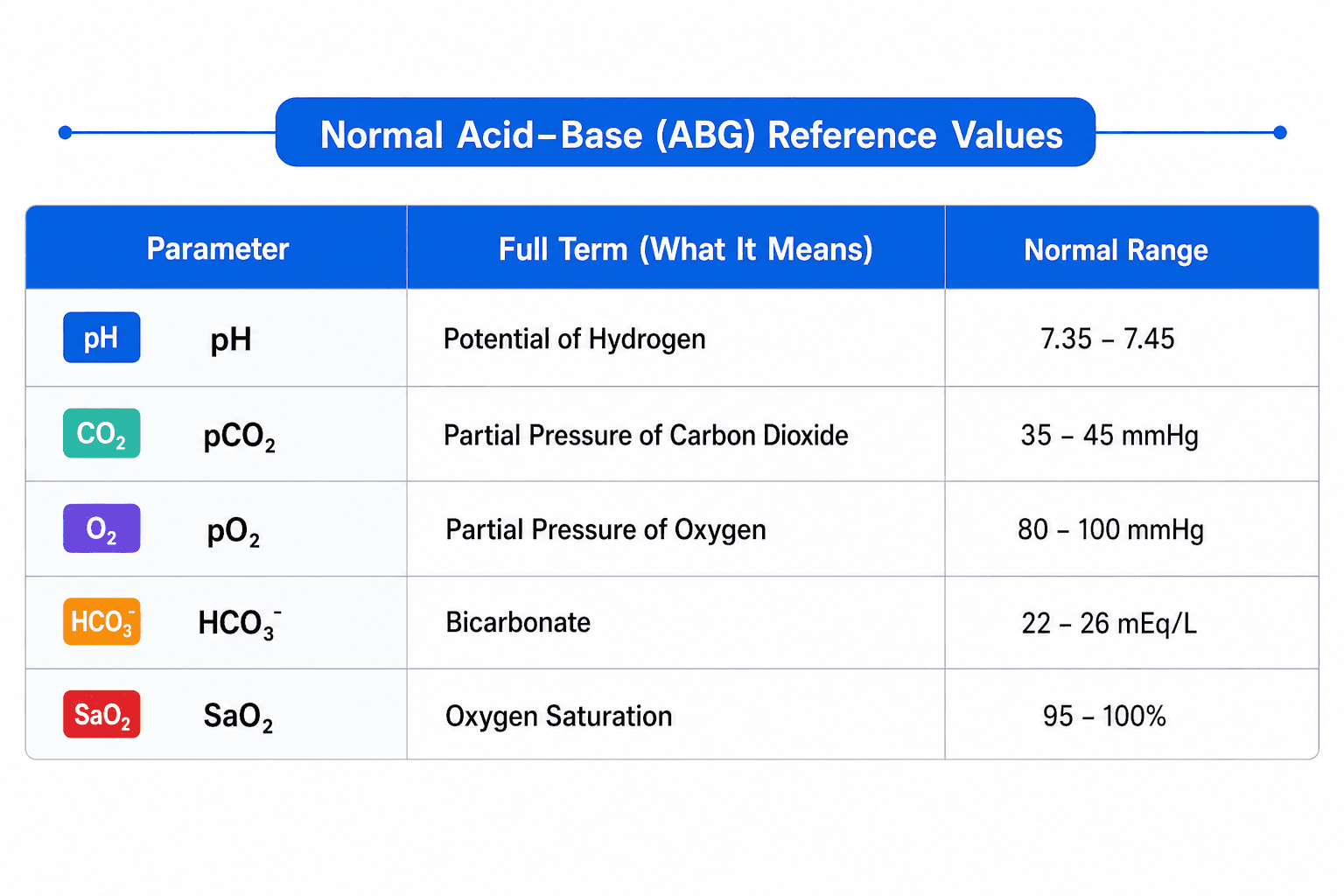
Two values drive most of your interpretation: pCO₂ (controlled by the lungs) and HCO₃ (controlled by the kidneys). pH tells you the result of what those two are doing.
One important note: certain chronic conditions allow clients to live comfortably with values slightly outside these ranges.
When Balance Breaks Down
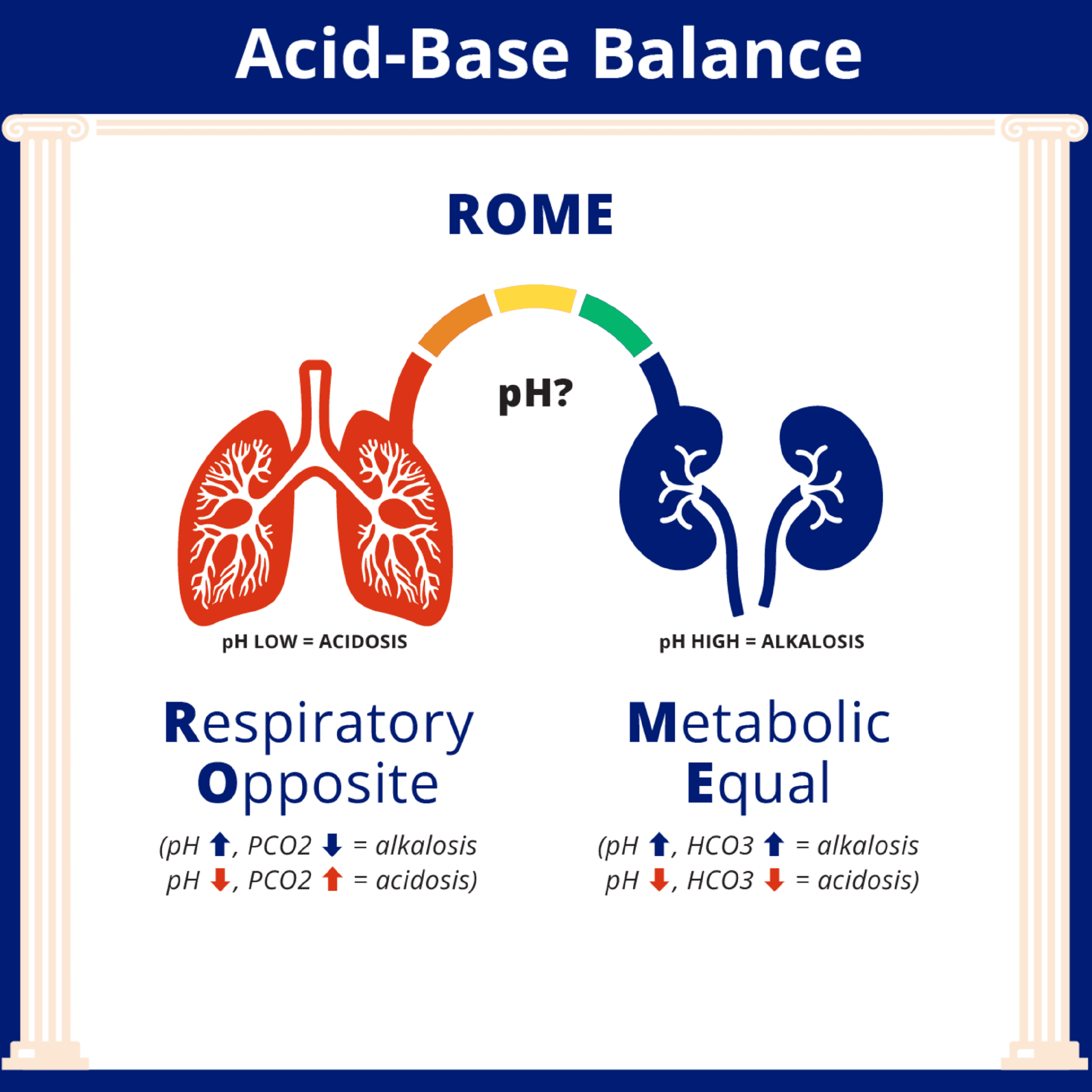
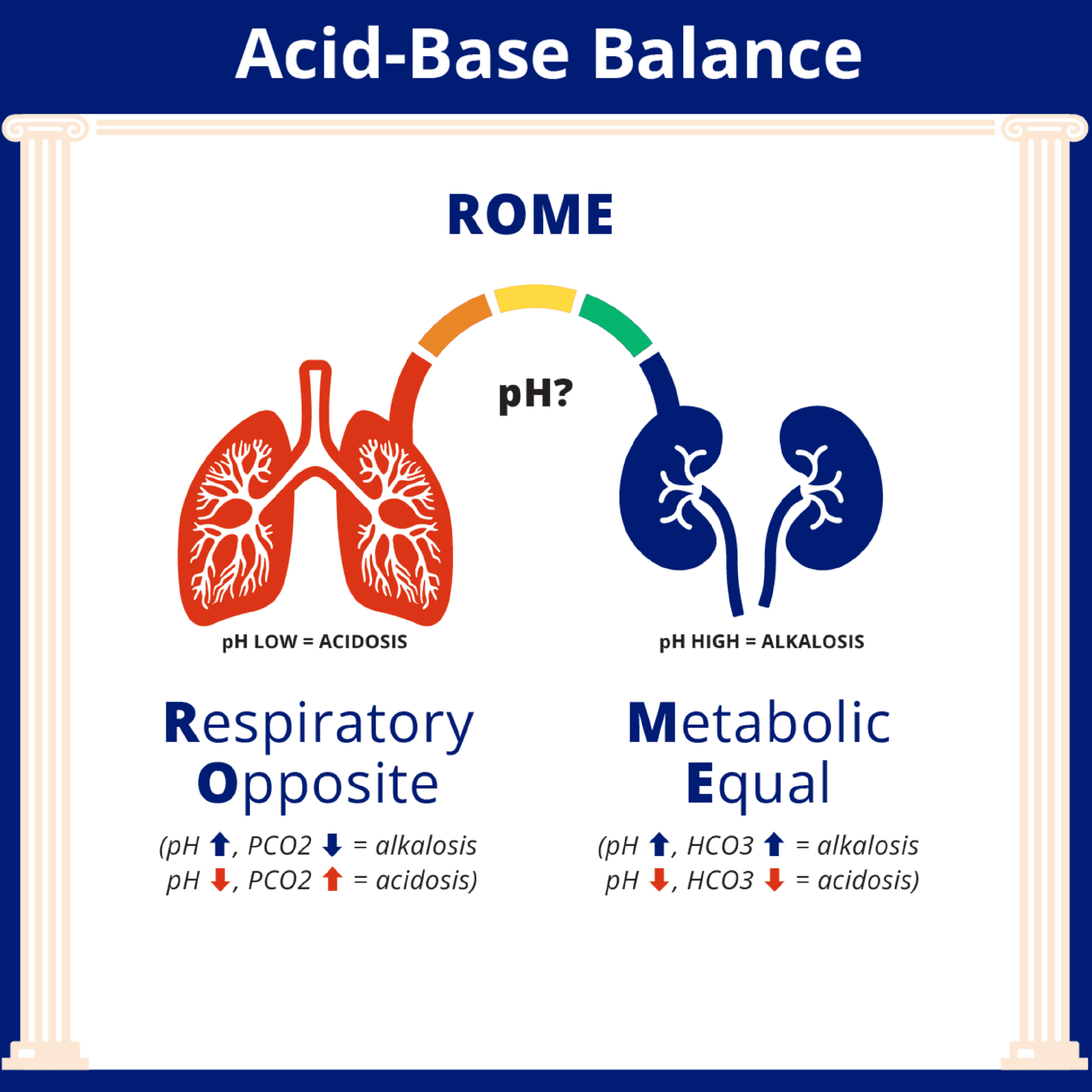
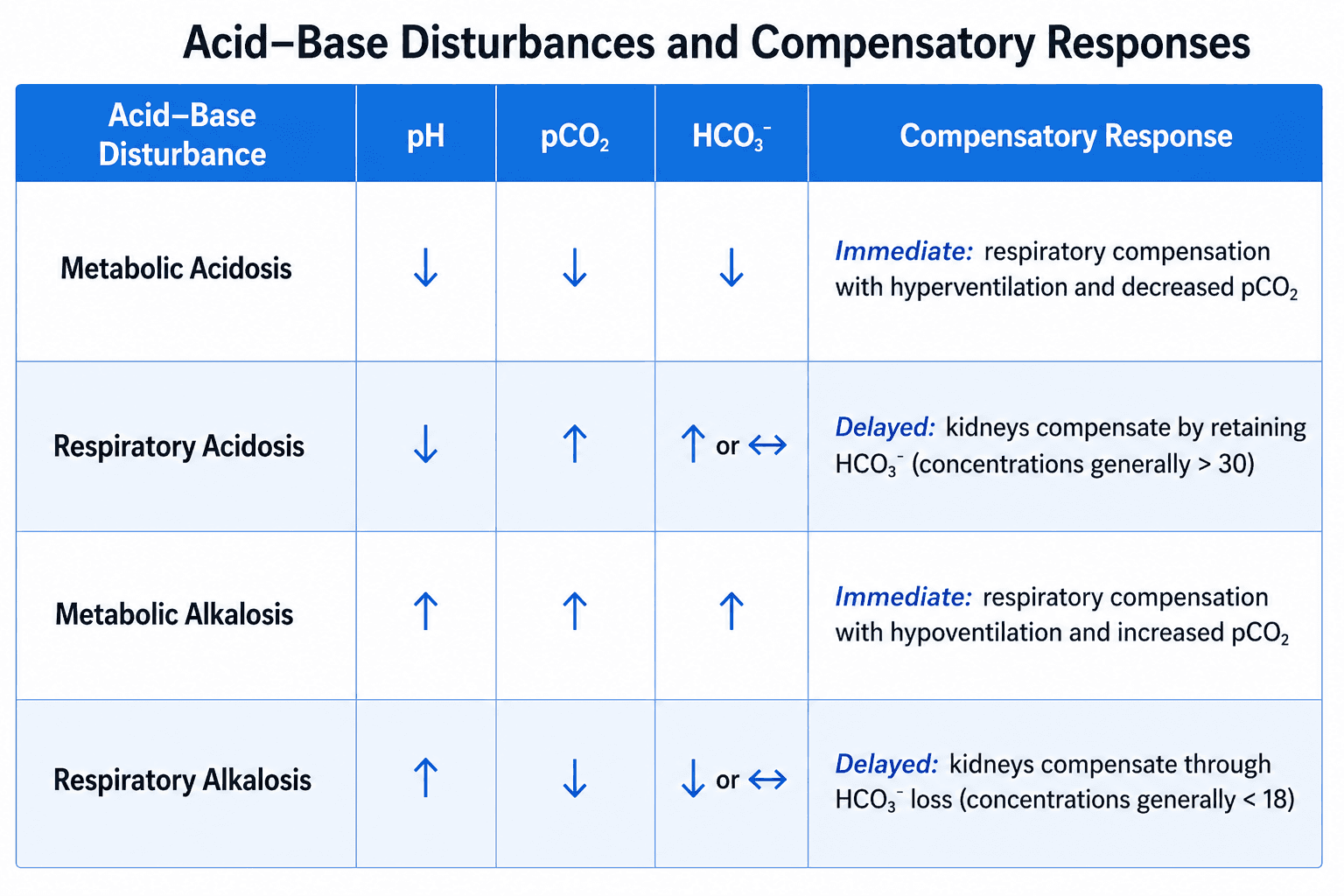
When the system tips out of range, the client develops either acidosis (pH below 7.35) or alkalosis (pH above 7.45). The cause is either respiratory or metabolic, which gives you four possible disorders:
Respiratory: pH and pCO₂ move in opposite directions
Metabolic: pH and HCO₃ move in the same direction
Respiratory acidosis happens when the lungs can't move air effectively and CO₂ builds up.
Think hypoventilation, COPD exacerbation, opioid overdose.
pH goes down, pCO₂ goes up.
Respiratory alkalosis happens when the client is breathing too fast and blowing off too much CO₂.
Think anxiety, hyperventilation, pain.
pH goes up, pCO₂ goes down.
Metabolic acidosis happens when the body accumulates acid or loses bicarbonate.
Think DKA, severe diarrhea, renal failure.
pH goes down, HCO₃ goes down.
Metabolic alkalosis happens when the body loses acid or retains too much bicarbonate.
Think prolonged vomiting, nasogastric suctioning, diuretic overuse.
pH goes up, HCO₃ goes up.
Clinical signs to know:
Acidosis depresses the central nervous system.
Look for lethargy, confusion, and decreased responsiveness.
Alkalosis excites the central nervous system.
Look for agitation, muscle twitching, and scattered thinking.
Acid makes you drowsy. Base makes you rowdy.
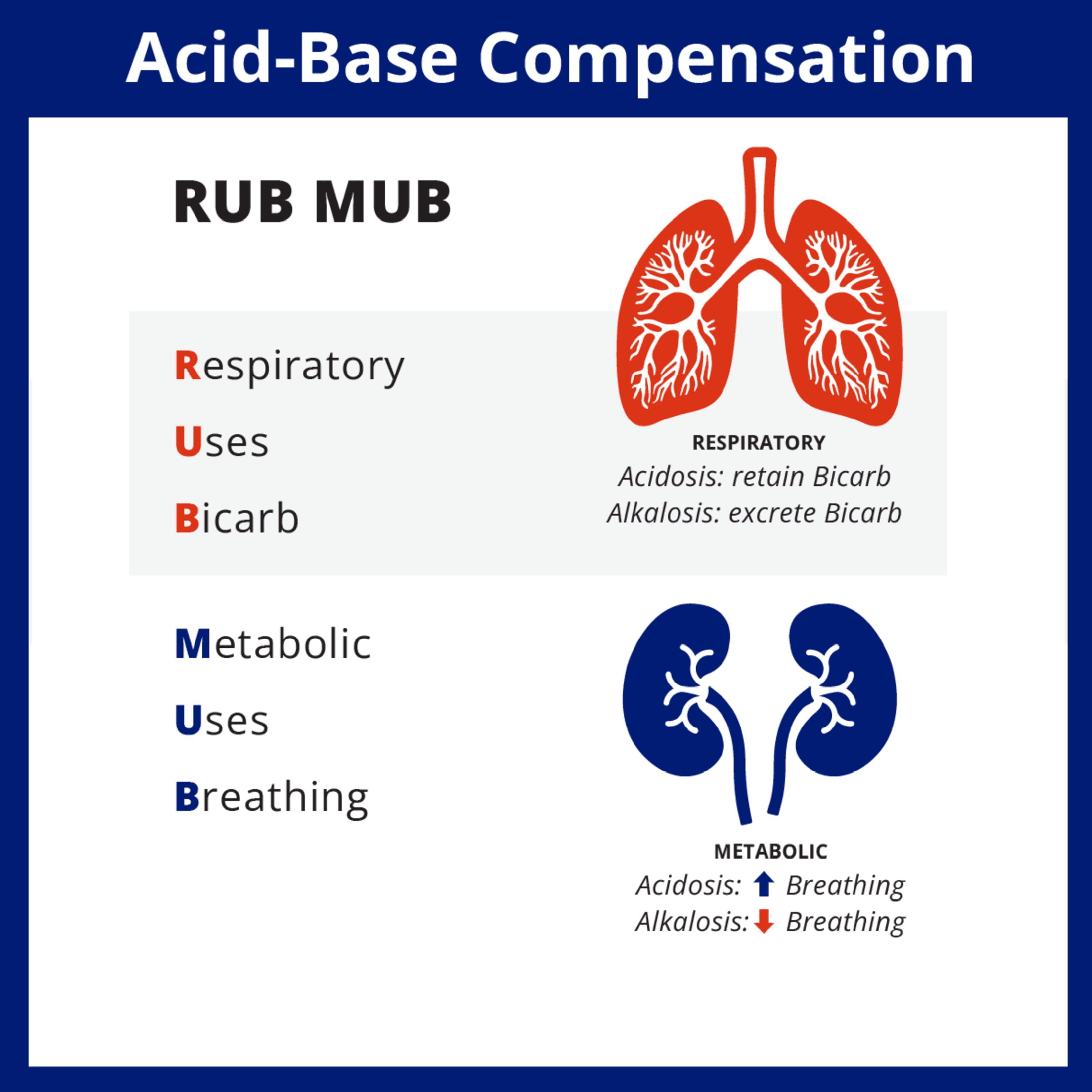
How the Body Fights Back
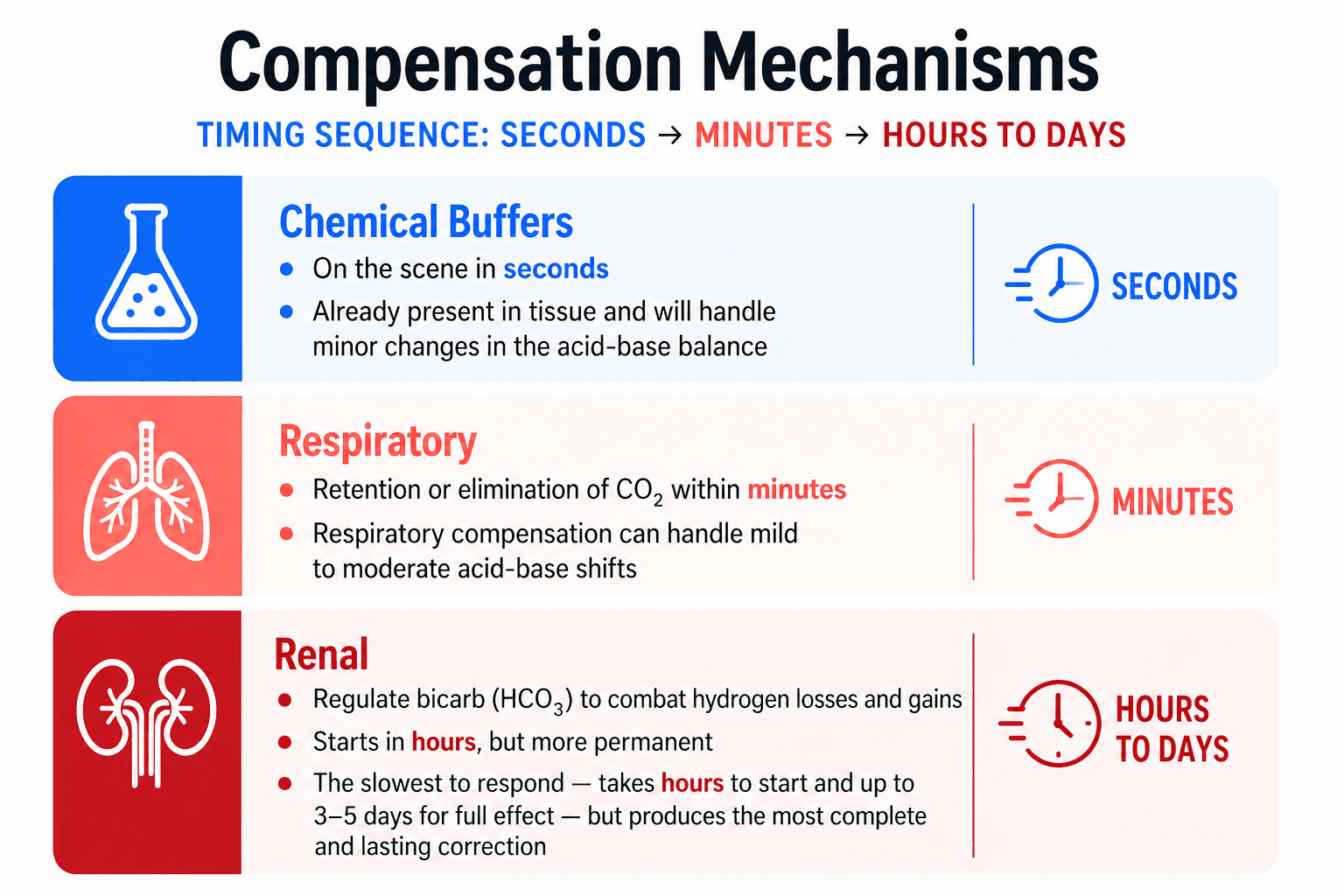
The body doesn't wait for you to intervene. The moment balance shifts, three mechanisms start working to correct it, each at a different speed.
Chemical buffers respond in seconds.
They're already present in the blood and tissues, ready to neutralize minor changes immediately.
Think of them as the first responders.
The respiratory system responds within minutes.
The lungs speed up or slow down breathing to adjust CO₂ levels.
This handles mild to moderate shifts, but it's not the final answer.
The kidneys respond over hours to days.
They regulate HCO₃ to manage hydrogen losses and gains.
The kidneys are the slowest to respond and take 3 to 5 days for full effect, but they produce the most complete and lasting correction.
Early, Partial, and Full Compensation
Understanding where a client is in this process changes what you're looking at on the ABG.
Early (uncompensated)
The primary disorder is present and the body hasn't mounted a meaningful response yet.
The pH is abnormal, and only one value (CO₂ or HCO₃) is out of range.
Example: pH 7.28, pCO₂ 55, HCO₃ 24.
That's respiratory acidosis without compensation started.
Middle (partially compensated)
The compensating system has activated but hasn't normalized the pH yet.
Now both CO₂ and HCO₃ are out of range, and the pH is moving toward normal but isn't there yet.
Example: pH 7.31, pCO₂ 55, HCO₃ 30.
The kidneys are retaining bicarb, but the pH is still low.
Late (fully compensated)
The pH has returned to normal range, but both CO₂ and HCO₃ are still abnormal.
The body has done the work.
Example: pH 7.38, pCO₂ 55, HCO₃ 32.
Respiratory acidosis, fully compensated.
Interpreting an ABG
Now that the NCLEX provides reference ranges on every question, you don't need to memorize the numbers. You need to know what to do with them. Here's the three-step approach:
Step 1: Look at the pH. Is it low (acidosis) or high (alkalosis)?
Step 2: Apply ROME. Look at CO₂ and HCO₃. Which one is moving in the wrong direction? That's your cause.
If CO₂ is the problem, it's respiratory.
If HCO₃ is the problem, it's metabolic.
Step 3: Check for compensation. Is the pH back to normal? If yes, fully compensated. Still abnormal but moving? Partially compensated. pH abnormal with only one value off? Not compensated yet.
Once you've identified the disorder, the question will ask you what to do next.
Nursing Care
For respiratory acidosis: the priority is ventilation. Help the client breathe, reposition, prepare for potential respiratory support.
For metabolic acidosis: address the underlying cause and support bicarbonate levels. In DKA, that means fluids and insulin, not direct bicarb replacement.
For metabolic alkalosis: replace fluids and electrolytes. Chloride-responsive alkalosis (vomiting, NG suction) responds to IV saline. Potassium replacement is often needed alongside.
For respiratory alkalosis: slow the breathing rate and address the underlying cause. For a client hyperventilating from anxiety, calm reassurance and controlled breathing coaching are first-line.
A note on paper bag rebreathing: You may have learned that breathing into a paper bag treats hyperventilation by allowing the client to rebreathe CO₂. This technique is still referenced in many journals and textbooks. However, it is contraindicated when there is any possibility of cardiac event, hypoxia, pulmonary embolism, or unknown oxygenation status. In practice, controlled breathing coaching and treating the underlying cause are the safer first-line approaches.
After any intervention, you're watching three things:
the complete metabolic panel (CMP) for electrolyte changes and renal function
serial ABGs for the direction of acid-base correction
respiratory status for changes in ventilation
The goal isn't just naming the disorder. It's knowing what to do, and knowing whether it's working.
References
Callaham, M. (1989). Hypoxic hazards of traditional paper bag rebreathing in hyperventilating patients. Annals of Emergency Medicine, 18(6), 622–628. https://doi.org/10.1016/S0196-0644(89)80515-3
Three documented deaths from misapplication of breathing in a paper bag; prompted the formal study showing dangerous O₂ drops within 60–90 seconds of rebreathing.
Saguil, A., & Fargo, M. V. (2015). Evaluation and management of hyperventilation syndrome. American Family Physician, 91(7), 470–474.
Conservative clinical guidance on treating hyperventilation; supports coaching and addressing underlying cause as first-line over rebreathing techniques.
Medscape. (2024). Hyperventilation syndrome treatment and management. https://emedicine.medscape.com/article/807277-treatment
Current clinical summary; explicitly states paper bag rebreathing is no longer recommended and cites documented deaths in patients with MI, pneumothorax, and PE.
National Council of State Boards of Nursing. (2026). 2026 NCLEX-RN test plan. NCSBN. https://www.nclex.com/files/2026_RN_Test%20Plan_English-F.pdf
Source for Physiological Adaptation category scope and Bloom's taxonomy framing.
Hall, J. E., & Hall, M. E. (2021). Guyton and Hall textbook of medical physiology (14th ed.). Elsevier.
Standard reference for the three-mechanism compensation model (chemical buffers, respiratory, renal) and associated timing.
Porth, C. M. (2015). Essentials of pathophysiology: Concepts of altered health states (4th ed.). Wolters Kluwer.
Supporting reference for acid-base disorder classification, compensation physiology, and CNS symptom profiles.

Kristin Everhart, MSN, ARNP, FNP-C
\
5 Study Strategies That Actually Work for the FNP Certification Exam
5 Study Strategies That Actually Work for the FNP Certification Exam

Kristin Everhart, MSN, ARNP, FNP-C
\
FNP Exam: Mastering Cardiology, Pharmacology, and Endocrinology




