Ben OConnor, BSN
\
03/2/2025

Nurses often see clients that have renal insufficiency, so we need to consider it every time we give a medication, send clients for diagnostic testing, provide IV fluids, or develop a care plan. This area of nursing is key to providing safe care. In fact, many clients develop acute kidney injury (AKI) as a result of hospital care.
So why is AKI such a huge part of nursing practice?
As a urology nurse, I recall a provider telling me that as soon as we are born, we begin to lose kidney function, kind of like wear and tear for car tires. I understood the point. It’s normal for function in a healthy kidney to decline with age, slowly, over many decades. If we take good care of our kidneys, they will function well.
With advanced healthcare, the percentage of those living later in life with one or more chronic conditions has been on the rise. So, chronic renal insufficiency, end-stage renal disease, or acute kidney injury make up a large workload for nurses in every healthcare setting.
The Power of Prevention
Understanding basics about kidney anatomy is helpful for mastering renal failure types. Determining the type of failure is directly connected to how it’s treated.
A kidney is similar to any filtering system. Blood flows into each kidney by way of large renal arteries and travels through a series of smaller and smaller vessels creating pressure.
This presses blood through the “filter,” called a glomerulus. Each glomerulus is surrounded by capillaries. (It’s a bit like making coffee, right?)
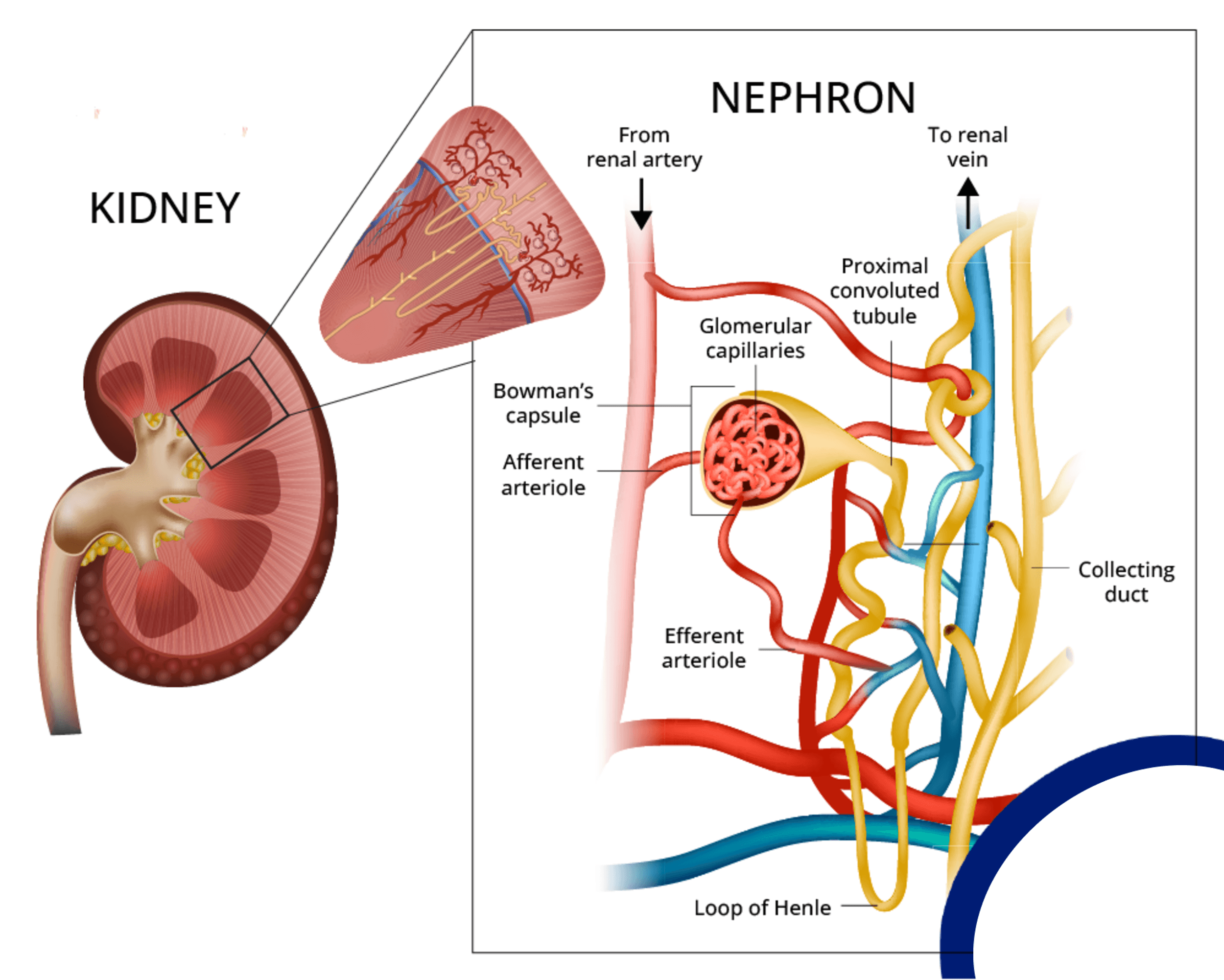
The rate at which blood is filtered is the glomerular filtration rate (GFR). Now, you don't have to know GFR for passing the NCLEX, but you must memorize normal values for two other kidney markers: BUN and creatinine.
At the cellular level, blood entering the kidney passes by membranes that allow the exchange of electrolytes and waste products, which are converted to urine. This an oversimplified view, but it’s all you need to tackle the tougher concepts.
Acute kidney injury leads to a rapid decrease in GFR (filtering slows) which leaves waste products in the blood. Because the kidney cannot regulate ion concentration (electrolytes), the client develops metabolic acidosis: low pH with a low bicarb.
Abnormally high nitrogen compounds and waste products such as urea and creatinine in the blood is a condition called azotemia.
AKI Phases
Early renal failure may include signs of compensation. Renal vessels constrict, and the renin-aldosterone-angiotensin system is activated. This causes antidiuretic hormone to resorb water and sodium.
Each phase of renal failure has different signs. Identifying the phase is a starting point.
Oliguria signals marked decreased output and electrolyte disturbances; serum BUN and creatinine rise.
Diuresis is abrupt onset of increased output (up to 10 L per day).
The last phase is called recovery.
Always identify whether there is oliguria or diuresis by checking output and urine specific gravity (urine concentration).
Regardless of which phase you find a patient in, watch for deterioration before acidosis occurs, and check for elevated urine protein, which indicates kidney damage. Large proteins abnormally leak into the urine. Sustained damage is called acute tubular necrosis.
Determine what type of AKI the client has. There are three types.
Prerenal AKI: Decreased Renal Artery Blood Flow
The goal is to prevent or treat electrolyte and fluid imbalance.
Picture kidney anatomy and imagine a problem that affects blood supply into the kidney. Think of a garden hose being pinched off before it reaches the sprinkler.
A problem occurs before blood is filtered and waste is removed, causing serious and sudden complications. It often occurs from hypovolemic shock. Be alert for potential causes of decreased renal blood flow, recognize clinical signs, and provide support before failure progresses.
This is the most common type of AKI for acutely ill clients and, in most cases, is reversible or preventable. Because the problem is outside of the kidney itself, nephrons (individual kidney cells) will still function once blood flow is restored.
However, if the client already has chronic renal disease, the kidney may not “bounce back” as it would in a previously healthy client.
Blocked arterial blood flow (obstruction): ruptured renal aneurysm, artery stenosis
Fluid loss (water supply to the “hose” is interrupted): diuretics, bleeding
Cardiogenic shock (decreased cardiac output): tamponade, heart failure
Signs and symptoms of pre-renal AKI:
Low BP, low MAP
Oliguria (under 400 mL per day)
Lethargy
Tips for Managing Prerenal AKI
It’s important to determine whether the kidney is still functioning by looking at urine sodium. Urine sodium tends to be low when there is a prerenal cause because the functioning kidney tries to compensate by retaining sodium.
The provider may order a fluid challenge (bolus), which is appropriate if the suspected cause is fluid loss. If the kidney is failing, sodium excretion increases.
Determine the phase. For oliguria, forcing large amounts of fluid will further stress the kidney.
Expect low-dose dopamine. At low doses, dopamine increases renal vasodilation. Studies disagree whether this can reverse renal failure, but the patient benefits from an increase in mean arterial pressure (MAP).
For complex clients, monitoring central venous pressure with a Swan-Ganz catheter is helpful.
Intrarenal AKI: Functional Problems
The goal is to optimize kidney function and prevent further damage.
In intrarenal AKI, or intrinsic AKI, the problem is inside the kidney, typically from chronic renal disease or acute damage to internal structures. This type is classified according to what part is affected:
Vascular: affecting small vessels (lupus, chronic HTN)
Glomerular or tubular: damage to the glomerulus or tubules (drug toxicity, IV contrast, infection, diabetes)
Interstitial: cellular level dysfunction (drug toxicity, sickle cell disease, low potassium levels, blood transfusion reaction)
Signs and symptoms of intra-renal AKI:
Hypertension, usually present in chronic disease, which worsens as damage worsens over 10–15 years or longer
Progressive inability to concentrate urine to oliguria
Tips for Managing Intrarenal AKI
Hemodialysis may be needed, especially if the client has anuria (defined as urine output less than 100 mL /day).
Urine studies often reveal red blood cell casts, proteinuria, and hematuria. A 24-hour urine test for protein helps diagnosis.
Postrenal AKI: Obstruction
The goal is to restore outflow asap.
This type is the easiest for nurses to understand because nurses manage urine output for so many client populations. When the kidney functions adequately, urine is produced and needs to exit the body.
Postrenal problems mean a blockage of urine trying to exit the body. This results in hydronephrosis, urine backing up into the ureters and kidney.
This type is also the easiest to correct in most cases but may require surgery. Obstruction may occur simply from a blocked catheter, so output assessment is a priority for clients with urinary diversion.
Obstructive AKI occurs either intrinsically (inside the kidney itself) or extrinsically (outside). Common intrinsic causes are kidney stones, blood clots, tumors, hypotonic (flaccid) bladder, anatomical problems (stricture), and inflammation.
Extrinsic obstructive AKI is outside the system, including structures that compress the ureter. An enlarged prostate is commonly the cause.
Signs and symptoms of post-renal failure:
Sudden onset anuria or marked fluctuation of urine volume, often intermittent but noticeable, including a change in urine stream or difficulty starting the urine stream
Depending on the cause, flank pain, dysuria, nausea, and urge to void
Urine backing up into the kidney, leading to lethargy, especially in the older client
Tips for Managing Postrenal AKI
Report urine output less than 30 mL/hr
Prolonged obstruction is a medical emergency. Focus on a solution that rapidly restores the exit of urine from the system. In many cases this involves temporary catheter insertion.
Priority AKI Assessment
Volume status: Watch for signs of fluid volume excess (FVE). Check orthostatic vital signs, look for jugular vein distention, third heart sounds, rales, ascites, and lower extremity edema.
Monitor intake and output.
Assess for bladder distention (make sure urine can exit the system).
Watch for edema caused by capillary leak (third spacing).
Track urine specific gravity and sodium.
Monitor blood -lytes. Kidney function affects serum K+, Ca+, phosphorus, and Na+.
AKI Expert Advice
Remember that worsening kidney function is defined by decreased rate of filtration. Clients may have oliguria, but they often have large amounts of dilute urine because the kidneys are not doing their job removing electrolytes and waste.
Sudden weight gain may be an early sign of renal failure.
For clients at risk for FVE, administer medications in the smallest volume possible.
Clients with severe kidney disease are not likely to respond to diuretics or may suffer damage from these drugs.
Signs of chronic renal disease are non-specific, meaning many conditions can cause the same symptoms. Always evaluate kidney function for all older clients.
Clients with AKI should avoid antacids with Mg, because because the kidneys have difficulty excreting Mg.
Increased respiratory rate is an early sign of fluid overload. Don’t forget to count respiratory rate when doing vital signs.

Catherine Cantrell, MSN, RN
\
Professional Communication: Email
Professional Communication: Email
Category

Catherine Cantrell, MSN, RN
\
One Small Mistake Nursing Students Make Taking the NCLEX—Don’t Let It Happen to YOU!
One Small Mistake Nursing Students Make Taking the NCLEX—Don’t Let It Happen to YOU!
Category

Catherine Cantrell, MSN, RN
\
What Happens If You Fail NCLEX 3 Times?



